Photos: Chad Hipolito/The Globe and Mail and Nicole Richard
The families fighting for action
Nicole Richard/Handout
It was a photo that stirred hearts across Canada: A group of 15 women who lost loved ones to drug overdoses posing together with crosses to illustrate the depth of the crisis – and to remind people that those who are dying “are somebody’s someone.”
The picture was circulated online by Moms Stop the Harm, a national organization lobbying for better drug policy. The group is calling on the federal government to declare the opioid crisis a national health emergency, to increase safe supply of drugs and to decriminalize possession of illicit substances.
The government response: The Liberals have repeatedly rejected calls to decriminalize possession of hard drugs. The party has said it will proceed on the issue of “safe supply” – that is, helping provide a regulated, quality-controlled source of drugs. The NDP and the Greens both support decriminalization. And while drug policy is a federal mandate, provinces and municipalities can take steps to de facto decriminalize. That’s what B.C.’s top public health officer is urging, but the NDP government has resisted the proposal.
Story continues below advertisement
Why decriminalization? Advocates say decriminalizing personal possession – a measure Portugal took in 2001 – would play a critical role in responding to the crisis. “The societal stigma associated with drug use leads many to use drugs alone and hidden, increasing their risk of dying. B.C. cannot ‘treat’ its way out of this overdose crisis, or ‘arrest’ its way out either,” health officer Bonnie Henry wrote in a report.
The Globe’s view: Our editorial board argues that decriminalization would be a key step in treating addiction as a health-care issue, not a criminal-law problem. “Decriminalization of drugs is not a magic bullet that will end drug addiction. But it can be part of a broader harm-reduction strategy that includes many other steps.”
Vancouver Fire and Rescue Services captain Jonathan Gormick and Vancouver Coastal Health social worker Robyn Kelway visit residences in Vancouver in August, 2019.
Jackie Dives/The Globe and Mail
How do you deliver services to drug users who are often hard to reach? A new outreach initiative in Vancouver pairs firefighters with social workers to follow up on recent overdose calls. At each location, a worker with Vancouver Fire and Rescue Services asks for the patient by name but says only that they’re following up on a recent call. If the patient is there and consents to further help, they wave over a Vancouver Coastal Health (VCH) social worker, who is waiting just out of sight.
The response: During an August trial period, the Combined Overdose Response Team made 107 visits, making contact in 22 of them, with 21 patients consenting to further help. That can include connecting people to housing supports or drug counsellors, and even teaching a user’s partner how to use a naloxone kit. “It doesn’t surprise me that they want help,” said Patricia Daly, chief medical health officer for VCH. “People don’t want to die; they want to get out of the cycle of repeated overdoses.”
The fly-in doctor
Dr. Todd Young, centre, and ‘recovery coach’ Craig Wiseman, right, carry charts and luggage off a small airstrip in the rain after landing in Clarenville, Nfld.
Darren Calabrese
For many patients in far-flung Newfoundland and Labrador towns, Todd Young is the only person who will prescribe opioid-replacement medication – and he flies his own plane to get to them. Dr. Young heads to eight-and-counting towns each month to provide access to methadone or Suboxone, allowing patients to receive help within five days as opposed to waits of one month or more in other rural parts of the province. Dr. Young manages about 600 patients that range in age from 15 to 94.
A long way to go: “This is not a popular form of medicine in Newfoundland,” said Dr. Young, who said many physicians “look at addictions patients as problem patients.” It’s not uncommon for him to show up to work to find a patient who has hitchhiked hundreds of kilometres to beg for treatment, or another waiting in her truck before office hours begin, trembling with the onset of withdrawal and the determination to get help. Dr. Young hopes that his willingness to treat addictions will eventually entice other physicians.
A multilayered response
Yellow boxes to dispose of used needles are now a fixture in Brantford.
Fred Lum/The Globe and Mail
As Brantford’s hospital admissions for overdoses soared in 2016 and 2017, leaders in the Southwestern Ontario city knew they had to act. Police Chief Geoff Nelson huddled with other local officials and put together a plan. Start treating users as sick people rather than criminals; make it easier for them to get addiction treatment; spread the word about the dangers of fentanyl; hand out lots of free naloxone kits.
Story continues below advertisement
Promising results: Although officials are quick to say the crisis is far from over, overdose figures were down sharply in 2018 from their peak in 2017. Emergency services responded to 35 per cent fewer overdose incidents in 2018. The hospital emergency department received 44 per cent fewer overdose visits.
PHS Community Services Society medical director Christy Sutherland said the idea to dispense hydromorphone in tablet form came from patients themselves, who were not satisfied with the injectable program.
B.C. has been the hardest-hit province in the overdose crisis, but it has also paved the way with innovative responses. Insite, North America’s first supervised consumption site, opened in Vancouver in 2003. Today, there are dozens of supervised sites across the country. There are also newer initiatives under way to stanch overdoses:
Pharmaceutical-grade pills: A pilot project from Vancouver’s largest social-service provider is allowing about 50 patients at a time to access the opioid hydromorphone in tablet form and ingest them on site while staff observe them. Hydromorphone is an opioid medication used to treat moderate to severe pain that is commonly used in palliative and acute care. One Vancouver study found that hydromorphone could be an affordable and effective substitution therapy for heroin.
Fighting fentanyl with fentanyl: A program launched in July, 2019, sees patients get a fentanyl patch – commonly used to treat chronic pain for conditions such as cancer – that is applied to the skin and changed every two days by a nurse. To address misuse, the patches are signed and dated, and a transparent film is applied to prevent tampering. It is believed to be the first formal program of its kind.
A proposal for regulated retail heroin sales: British Columbia’s authority on addictions care is recommending allowing regulated retail heroin sales in the province to reduce overdose deaths caused by fentanyl-tainted illicit drugs and to generate funds for addiction-treatment services. Members would be permitted to purchase personal amounts of the drug from a location connected to health-care services.
Sam Stahnke was making good money working three weeks a month in Alberta’s oil sands. Then a knee injury forced him to go on opioid painkillers, and soon he was buying Oxycontin, hydromorphone and morphine pills by the thousands. Soon, he started crushing the pills into powder, mixing it with saline solution and injecting the liquid with a big syringe. Then, he turned to heroin. But he kept working, never telling anyone as he used drugs in the isolation of his house in Campbell River, B.C. “I’m lucky to be alive,” he says, recalling the years before his recovery.
The ‘working-man’s code’: B.C. statistics show that of those who died by overdose that were employed, 55 per cent worked in transport or the trades. In Ontario, one-third with known employment status were in construction. The vast majority of victims are men, and most die in private residences. But stigma remains pervasive, with working men reluctant to seek help. “This has been a neglected population that nobody is talking about,” says Andrea Furlan, a scientist at the Institute for Work and Health in Toronto.
Addressing the problem: Authorities have been aware of the issue for trades workers for years, but action has been slow. Mr. Stahnke found the courage to tell his family doctor, and was put on Suboxone, a substitute opioid that reduces the craving for drugs without producing a high. He hopes that telling his story will encourage others in his position to get help.
The prison system
One of the letters sent by Spencer Kell to his friend Manie Daniels.
Tijana Martin/The Globe and Mail
When Spencer Kell got out of jail in the spring of 2018, leaving his cellmate Manie Daniels behind, the two friends started exchanging letters. Both had used drugs in the past; they shared their struggles – and hopes – in the notes. The pair hoped to reunite soon after Daniels’s release that July. “I’m waiting for you! Write me soon. Stay safe,” Mr. Kell wrote. But Daniels died less than two days after getting out, overdosing on hydromorphone.
Transitioning to civilian life: Mr. Kell told a Senate forum in February, 2019, that with nowhere else to go, just-released prisoners often head “right back to the dealer’s house.” The numbers bear that out: A study on overdose deaths in Ontario showed that, between 2006 and 2013, one in 10 happened within a year of release from a provincial jail.
The services available: After his release, Mr. Kell ended up at the Salvation Army’s Ottawa Booth Centre, a Christian non-profit that offers help to the capital’s homeless and the addicted. He subsequently found an apartment and finished a college course on becoming an addiction worker. In Ontario, when prisoners are released they get naloxone kits and training about how to use the overdose-reversal drug, as well as a wallet card on how to avoid an opioid overdose. But the families of victims say that’s not nearly enough. They are advocating for more treatment programs and beds.
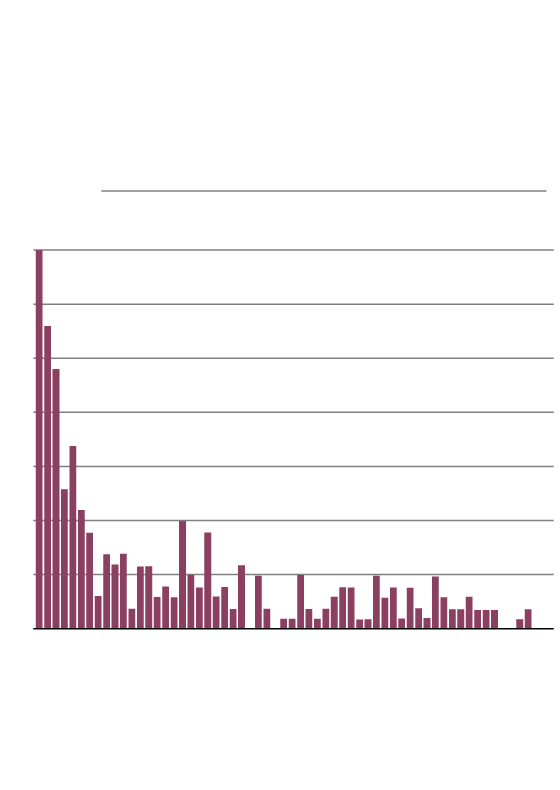
ontario Drug Toxicity Deaths
after incarceration
Number of deaths by day in the year after release from provincial incarceration, up to day 60, 2006–2013.
Days since release from incarceration
JOHN SOPINSKI/THE GLOBE AND MAIL
SOURCE: pols.org
ontario Drug Toxicity Deaths
after incarceration
Number of deaths by day in the year after release from provincial incarceration, up to day 60, 2006–2013.
Days since release from incarceration
JOHN SOPINSKI/THE GLOBE AND MAIL, SOURCE: pols.org
ontario Drug Toxicity Deaths after incarceration
Number of deaths by day in the year after release from provincial incarceration, up to day 60, 2006–2013.
Days since release from incarceration
JOHN SOPINSKI/THE GLOBE AND MAIL, SOURCE: pols.org
Compiled by Arik Ligeti, based on reports from Marcus Gee, Andrea Woo and Jessica Leeder
Story continues below advertisement
Our Morning Update and Evening Update newsletters are written by Globe editors, giving you a concise summary of the day’s most important headlines. Sign up today.
Skinstitut Holiday Gift Kits take the stress out of gifting
Toronto, October 31, 2024 – Beauty gifts are at the top of holiday wish lists this year, and Laser Clinics Canada, a leader in advanced beauty treatments and skincare, is taking the pressure out of seasonal shopping. Today, Laser Clincs Canada announces the arrival of its 2024 Holiday Gift Kits, courtesy of Skinstitut, the exclusive skincare line of Laser Clinics Group.
In time for the busy shopping season, the limited-edition Holiday Gifts Kits are available in Laser Clinics locations in the GTA and Ottawa. Clinics are conveniently located in popular shopping centers, including Hillcrest Mall, Square One, CF Sherway Gardens, Scarborough Town Centre, Rideau Centre, Union Station and CF Markville. These limited-edition Kits are available on a first come, first served basis.
“These kits combine our best-selling products, bundled to address the most relevant skin concerns we’re seeing among our clients,” says Christina Ho, Senior Brand & LAM Manager at Laser Clinics Canada. “With several price points available, the kits offer excellent value and suit a variety of gift-giving needs, from those new to cosmeceuticals to those looking to level up their skincare routine. What’s more, these kits are priced with a savings of up to 33 per cent so gift givers can save during the holiday season.
There are two kits to select from, each designed to address key skin concerns and each with a unique theme — Brightening Basics and Hydration Heroes.
Brightening Basics is a mix of everyday essentials for glowing skin for all skin types. The bundle comes in a sleek pink, reusable case and includes three full-sized products: 200ml gentle cleanser, 50ml Moisture Defence (normal skin) and 30ml1% Hyaluronic Complex Serum. The Brightening Basics kit is available at $129, a saving of 33 per cent.
Hydration Heroes is a mix of hydration essentials and active heroes that cater to a wide variety of clients. A perfect stocking stuffer, this bundle includes four deluxe products: Moisture 15 15 ml Defence for normal skin, 10 ml 1% Hyaluronic Complex Serum, 10 ml Retinol Serum and 50 ml Expert Squalane Cleansing Oil. The kit retails at $59.
In addition to the 2024 Holiday Gifts Kits, gift givers can easily add a Laser Clinic Canada gift card to the mix. Offering flexibility, recipients can choose from a wide range of treatments offered by Laser Clinics Canada, or they can expand their collection of exclusive Skinstitut products.
Brightening Basics 2024 Holiday Gift Kit by Skinstitut, available exclusively at Laser Clincs Canada clinics and online at skinstitut.ca.
Hydration Heroes 2024 Holiday Gift Kit by Skinstitut – available exclusively at Laser Clincs Canada clinics and online at skinstitut.ca.
LONDON (AP) — Most people have accumulated a pile of data — selfies, emails, videos and more — on their social media and digital accounts over their lifetimes. What happens to it when we die?
It’s wise to draft a will spelling out who inherits your physical assets after you’re gone, but don’t forget to take care of your digital estate too. Friends and family might treasure files and posts you’ve left behind, but they could get lost in digital purgatory after you pass away unless you take some simple steps.
Here’s how you can prepare your digital life for your survivors:
Apple
The iPhone maker lets you nominate a “ legacy contact ” who can access your Apple account’s data after you die. The company says it’s a secure way to give trusted people access to photos, files and messages. To set it up you’ll need an Apple device with a fairly recent operating system — iPhones and iPads need iOS or iPadOS 15.2 and MacBooks needs macOS Monterey 12.1.
For iPhones, go to settings, tap Sign-in & Security and then Legacy Contact. You can name one or more people, and they don’t need an Apple ID or device.
You’ll have to share an access key with your contact. It can be a digital version sent electronically, or you can print a copy or save it as a screenshot or PDF.
Take note that there are some types of files you won’t be able to pass on — including digital rights-protected music, movies and passwords stored in Apple’s password manager. Legacy contacts can only access a deceased user’s account for three years before Apple deletes the account.
Google
Google takes a different approach with its Inactive Account Manager, which allows you to share your data with someone if it notices that you’ve stopped using your account.
When setting it up, you need to decide how long Google should wait — from three to 18 months — before considering your account inactive. Once that time is up, Google can notify up to 10 people.
You can write a message informing them you’ve stopped using the account, and, optionally, include a link to download your data. You can choose what types of data they can access — including emails, photos, calendar entries and YouTube videos.
There’s also an option to automatically delete your account after three months of inactivity, so your contacts will have to download any data before that deadline.
Facebook and Instagram
Some social media platforms can preserve accounts for people who have died so that friends and family can honor their memories.
When users of Facebook or Instagram die, parent company Meta says it can memorialize the account if it gets a “valid request” from a friend or family member. Requests can be submitted through an online form.
The social media company strongly recommends Facebook users add a legacy contact to look after their memorial accounts. Legacy contacts can do things like respond to new friend requests and update pinned posts, but they can’t read private messages or remove or alter previous posts. You can only choose one person, who also has to have a Facebook account.
You can also ask Facebook or Instagram to delete a deceased user’s account if you’re a close family member or an executor. You’ll need to send in documents like a death certificate.
TikTok
The video-sharing platform says that if a user has died, people can submit a request to memorialize the account through the settings menu. Go to the Report a Problem section, then Account and profile, then Manage account, where you can report a deceased user.
Once an account has been memorialized, it will be labeled “Remembering.” No one will be able to log into the account, which prevents anyone from editing the profile or using the account to post new content or send messages.
X
It’s not possible to nominate a legacy contact on Elon Musk’s social media site. But family members or an authorized person can submit a request to deactivate a deceased user’s account.
Passwords
Besides the major online services, you’ll probably have dozens if not hundreds of other digital accounts that your survivors might need to access. You could just write all your login credentials down in a notebook and put it somewhere safe. But making a physical copy presents its own vulnerabilities. What if you lose track of it? What if someone finds it?
Instead, consider a password manager that has an emergency access feature. Password managers are digital vaults that you can use to store all your credentials. Some, like Keeper,Bitwarden and NordPass, allow users to nominate one or more trusted contacts who can access their keys in case of an emergency such as a death.
But there are a few catches: Those contacts also need to use the same password manager and you might have to pay for the service.
___
Is there a tech challenge you need help figuring out? Write to us at onetechtip@ap.org with your questions.
The Canadian Paediatric Society says doctors should regularly screen children for reading difficulties and dyslexia, calling low literacy a “serious public health concern” that can increase the risk of other problems including anxiety, low self-esteem and behavioural issues, with lifelong consequences.
New guidance issued Wednesday says family doctors, nurses, pediatricians and other medical professionals who care for school-aged kids are in a unique position to help struggling readers access educational and specialty supports, noting that identifying problems early couldhelp kids sooner — when it’s more effective — as well as reveal other possible learning or developmental issues.
The 10 recommendations include regular screening for kids aged four to seven, especially if they belong to groups at higher risk of low literacy, including newcomers to Canada, racialized Canadians and Indigenous Peoples. The society says this can be done in a two-to-three-minute office-based assessment.
Other tips encourage doctors to look for conditions often seen among poor readers such as attention-deficit hyperactivity disorder; to advocate for early literacy training for pediatric and family medicine residents; to liaise with schools on behalf of families seeking help; and to push provincial and territorial education ministries to integrate evidence-based phonics instruction into curriculums, starting in kindergarten.
Dr. Scott McLeod, one of the authors and chair of the society’s mental health and developmental disabilities committee, said a key goal is to catch kids who may be falling through the cracks and to better connect families to resources, including quicker targeted help from schools.
“Collaboration in this area is so key because we need to move away from the silos of: everything educational must exist within the educational portfolio,” McLeod said in an interview from Calgary, where he is a developmental pediatrician at Alberta Children’s Hospital.
“Reading, yes, it’s education, but it’s also health because we know that literacy impacts health. So I think that a statement like this opens the window to say: Yes, parents can come to their health-care provider to get advice, get recommendations, hopefully start a collaboration with school teachers.”
McLeod noted that pediatricians already look for signs of low literacy in young children by way of a commonly used tool known as the Rourke Baby Record, which offers a checklist of key topics, such as nutrition and developmental benchmarks, to cover in a well-child appointment.
But he said questions about reading could be “a standing item” in checkups and he hoped the society’s statement to medical professionals who care for children “enhances their confidence in being a strong advocate for the child” while spurring partnerships with others involved in a child’s life such as teachers and psychologists.
The guidance said pediatricians also play a key role in detecting and monitoring conditions that often coexist with difficulty reading such as attention-deficit hyperactivity disorder, but McLeod noted that getting such specific diagnoses typically involves a referral to a specialist, during which time a child continues to struggle.
He also acknowledged that some schools can be slow to act without a specific diagnosis from a specialist, and even then a child may end up on a wait list for school interventions.
“Evidence-based reading instruction shouldn’t have to wait for some of that access to specialized assessments to occur,” he said.
“My hope is that (by) having an existing statement or document written by the Canadian Paediatric Society … we’re able to skip a few steps or have some of the early interventions present,” he said.
McLeod added that obtaining specific assessments from medical specialists is “definitely beneficial and advantageous” to know where a child is at, “but having that sort of clear, thorough assessment shouldn’t be a barrier to intervention starting.”
McLeod said the society was partly spurred to act by 2022’s “Right to Read Inquiry Report” from the Ontario Human Rights Commission, which made 157 recommendations to address inequities related to reading instruction in that province.
He called the new guidelines “a big reminder” to pediatric providers, family doctors, school teachers and psychologists of the importance of literacy.
“Early identification of reading difficulty can truly change the trajectory of a child’s life.”
This report by The Canadian Press was first published Oct. 23, 2024.