When schools reopened in Ottawa on Feb. 1, so many people logged on to public health’s online COVID-19 symptom quiz that the server crashed.
Author of the article:
Jacquie Miller
Publishing date:
Feb 17, 2021 • 12 hours ago • 7 minute read
Students returned to in-class learning Fe. 1 at Vincent Massey Public School in Ottawa. Photo by BLAIR GABLE /REUTERS
Article content
When schools reopened in Ottawa on Feb. 1, so many people logged on to public health’s online COVID-19 symptom quiz that the server crashed.
“It was bittersweet”, laughs Dr. Nisha Thampi, a pediatric infectious diseases specialist at CHEO.
“We don’t want families to be frustrated in doing the right thing. But that (crash) just speaks to the renewed energy in our community to do right by our children, and by our other families, and our neighbours.”
Daily screening, along with self-isolation and testing, are key components of efforts to keep COVID-19 out of schools, especially as more contagious variants of the virus take hold in Ontario.
It’s not always easy to sort through what constitutes doing the right thing in any of those key areas, though.
The rules keep changing and vary across the province. Messages from local and provincial authorities can conflict. It’s complicated, from what type of cough triggers a COVID-19 high alert to whether siblings without symptoms should stay home from school.
Advertisement
Story continues below
This advertisement has not loaded yet, but your article continues below.
Article content
And underlying all of those issues is the reality that it’s easier for some families than others to follow public health guidance.
For those with precarious employment it may mean a choice between doing the right thing by self-isolating at home or losing a job or the wages needed to pay the rent or buy groceries, says Thampi.
COVID-19 prevention guidelines are weakened in the absence of sick or other paid leave to help families comply with them, she points out.
Here’s a rundown of the latest rules:
Daily screening for symptoms
Staff and students are expected to screen themselves every day before school with a series of questions about symptoms of illness, travel history and close contacts. High school students must confirm they’ve passed the quiz — usually verbally to a teacher at school.
The symptom categories are similar. Symptoms that are less associated with COVID-19 — a runny nose, nausea, vomiting and diarrhea, tiredness or muscle aches, sore throat and headaches — are grouped in one category. Students with one of those symptoms are advised to stay home for 24 hours, but if symptoms improve they can go back to school.
Students who have two of those symptoms, however, or one symptom from the no-go list — cough, fever, chills, shortness of breath or loss of taste or smell — are told to stay home and consult a doctor (Ontario screening tool) or immediately get a COVID test (Ottawa tool).
Advertisement
Story continues below
This advertisement has not loaded yet, but your article continues below.
Article content
COVID-19 testing lineup at Brewer Park testing centre in September.Photo by Julie Oliver /Postmedia
Screening is far from an exact science.
Symptoms that are related to some other condition, for instance, don’t necessarily count.
If a student has a runny nose that is probably allergies, extreme fatigue that might be depression or a cough that seems like asthma, they don’t have to check off those symptoms when using the tool.
If parents are asked by a school or daycare for more information about a child’s symptoms that may be attributable to another condition, OPH provides a form they can fill out.
However, as Ottawa Public Health also notes, “having an underlying condition does not necessarily mean that your child does not also have COVID-19.”
And sorting symptoms into two categories is based on the best available evidence but means some COVID-19 cases will slip through.
Most children and youth with COVID-19 have no symptoms at all or only mild ones.
And there is a large variation in signs and symptoms of COVID-19 in children, note the medical experts who contributed to an Ontario school reopening report co-ordinated by SickKids hospital in Toronto.
“Predominant symptoms have included fever and cough in more than half the cases, followed by runny nose/nasal congestion, myalgia/fatigue and sore throat in 10–20 per cent of cases and gastrointestinal symptoms and headache in fewer than 10 per cent of cases,” says the report.
The self-screening test was stricter when schools opened in September. Any one symptom triggered a trip for a COVID-19 test, leading to hours-long lineups at overwhelmed assessment centres and days of waiting for appointments and results.
Advertisement
Story continues below
This advertisement has not loaded yet, but your article continues below.
Article content
The screening rules were relaxed on Oct. 1. The number of COVID-19 tests conducted on school-aged children immediately plummeted.
There is now a renewed debate over whether screening should be tightened again. The benefits of stricter screening in keeping COVID-19 out of schools have to be weighed against the disruption to kids and their families.
The SickKids report recommends a regional approach based on the level of community transmission of the virus.
In areas with “moderate to high” community transmission, the threshold for school exclusion and testing should be lower, such as single-symptom screening, said the report. Single-symptom school screening has already been adopted by the local public health units in the COVID-19 hot spots of Peel and Toronto.
Lower-risk areas may require a different approach.
In Renfrew County, for instance, which is currently in the “green” zone under the province’s colour-coded pandemic response guide, the public health unit does not support stricter screening.
“We need to balance the risk of transmission with the negative fallout for students and working parents from unnecessarily aggressive isolation procedures,” said a statement from the Renfrew County and District Health Unit.
“Schools, we have learned, are not significant drivers of infection and sending scores of kids with a runny nose home and isolating cases for up to 14 days is highly disruptive, so it has to be warranted.
Advertisement
Story continues below
This advertisement has not loaded yet, but your article continues below.
Article content
“In Renfrew County and District we sent over 600 kids and staff home to identify only seven additional (COVID-19) cases.”
There is also the logistical challenge of whether testing centres could meet the increased demand if screening is tightened.
Dr. David Williams, Ontario’s chief medical officer of healthjpg
Ontario Chief Medical Officer of Health Dr. David Williams has said he doesn’t want a return to the September testing logjams, which he describes as “very frustrating” for parents.
Who has to stay home and when
Anyone who fails the self-screening quiz must stay home and should get a COVID-19 test, says OPH.
Everyone in their household is also expected to self-isolate at home until the person with symptoms has a negative test result.
The rules are less clear in the case of people who do not have symptoms themselves but have been ordered to self-isolate because they have been in close contact with someone who has COVID-19. Close contacts must self-isolate for 14 days.
But do their asymptomatic household members have to self-isolate too?
The province says yes. Ottawa Public Health says no.
“The rest of the family do not need to be in isolation and do not need to be tested,” says OPH. As long as they have no symptoms, for instance, siblings can go to school and parents can go to work.
Ontario, in contrast, issued new guidelines in late January as part of its six-point plan to fight the spread of virus variants. “Households of all contacts and symptomatic individuals will be asked to stay home until the contact has received a negative test,” said the Ministry of Health in a statement.
Advertisement
Story continues below
This advertisement has not loaded yet, but your article continues below.
Article content
The different interpretations could affect thousands of families with school-aged children.
When someone at school contracts COVID-19, typically everyone in the class and cohort is identified as a close contact and sent home to isolate. Cohorts could include, for instance, students riding the same bus or attending the same before and after-school care.
On average, 20 high-risk contacts were identified for each school attendee who tested positive for COVID-19, according to a report by OPH that considered the time period of September, October and November. Schools opened gradually throughout September in Ottawa.
During that time, a total of 11,376 students and staff were identified as high-risk contacts, the report said.
The latest advice from OPH is that close contacts should be tested for COVID-19 on Day 7 of their 14-day isolation. The 14-day countdown starts from the day of exposure.
So if families follow the provincial guidelines, household members of a child sent home as a close contact could be in self-isolation for days while waiting for their child’s test result.
All about Testing
Ottawa public health officials say testing capacity has been ramped up. Same-day or next-day appointments are often available and results are usually ready in one or two days.
Students who pass the self-screening test but have a mild symptom can also be tested. In fact, OPH is encouraging it.
Here’s the message, in large bold type, on the OPH screening quiz: “please note it is possible that someone could test positive for COVID-19 even if they only have one symptom.
Advertisement
Story continues below
This advertisement has not loaded yet, but your article continues below.
Article content
“If you remain concerned that your child may have COVID-19 even though there is only one symptom, you may choose to have your child tested at an assessment centre.”
Testing is not mandatory for anyone. Students must follow public-health guidance on how long to self-isolate, but according to provincial guidelines are not required to show proof of a negative test to go back to school.
Hundreds of families with children waited in long, snaking lineups in the park outside Brewer Park COVID-19 testing centre on September 16, 2020Photo by Julie Oliver /Postmedia
Parents are sometimes reluctant to have their child tested because they fear the procedure will be uncomfortable or it’s difficult for them to get to a test site. Others may conclude that a test is unnecessary if the child has to stay home and self-isolate anyway.
Public health authorities strongly encourage testing.
It’s another case of doing the right thing — for the community, in this case.
“Testing is critical to our public health response — knowing how much the virus is circulating in the community, preventing further spread and getting the virus under control will help prevent further transmission and future lockdowns,” says OPH.
jmiller@postmedia.com
twitter.com/JacquieAMiller
Share this article in your social network
Ottawa Citizen Headline News
Sign up to receive daily headline news from Ottawa Citizen, a division of Postmedia Network Inc.
By clicking on the sign up button you consent to receive the above newsletter from Postmedia Network Inc. You may unsubscribe any time by clicking on the unsubscribe link at the bottom of our emails. Postmedia Network Inc. | 365 Bloor Street East, Toronto, Ontario, M4W 3L4 | 416-383-2300
Thanks for signing up!
A welcome email is on its way. If you don’t see it please check your junk folder.
The next issue of Ottawa Citizen Headline News will soon be in your inbox.
We encountered an issue signing you up. Please try again
Some Ontario doctors have started offering a free shot that can protect babies from respiratory syncytial virus while Quebec will begin its immunization program next month.
The new shot called Nirsevimab gives babies antibodies that provide passive immunity to RSV, a major cause of serious lower respiratory tract infections for infants and seniors, which can cause bronchiolitis or pneumonia.
Ontario’s ministry of health says the shot is already available at some doctor’s offices in Ontario with the province’s remaining supply set to arrive by the end of the month.
Quebec will begin administering the shots on Nov. 4 to babies born in hospitals and delivery centers.
Parents in Quebec with babies under six months or those who are older but more vulnerable to infection can also book immunization appointments online.
The injection will be available in Nunavut and Yukon this fall and winter, though administration start dates have not yet been announced.
This report by The Canadian Press was first published Oct. 21, 2024.
-With files from Nicole Ireland
Canadian Press health coverage receives support through a partnership with the Canadian Medical Association. CP is solely responsible for this content.
ISLAMABAD (AP) — Polio cases are rising ahead of a new vaccination campaign in Pakistan, where violence targeting health workers and the police protecting them has hampered years of efforts toward making the country polio-free.
Since January, health officials have confirmed 39 new polio cases in Pakistan, compared to only six last year, said Anwarul Haq of the National Emergency Operation Center for Polio Eradication.
The new nationwide drive starts Oct. 28 with the aim to vaccinate at least 32 million children. “The whole purpose of these campaigns is to achieve the target of making Pakistan a polio-free state,” he said.
Pakistan regularly launches campaigns against polio despite attacks on the workers and police assigned to the inoculation drives. Militants falsely claim the vaccination campaigns are a Western conspiracy to sterilize children.
Most of the new polio cases were reported in the southwestern Balochistan and southern Sindh province, following by Khyber Pakhtunkhwa province and eastern Punjab province.
The locations are worrying authorities since previous cases were from the restive northwest bordering Afghanistan, where the Taliban government in September suddenly stopped a door-to-door vaccination campaign.
Afghanistan and Pakistan are the two countries in which the spread of the potentially fatal, paralyzing disease has never been stopped. Authorities in Pakistan have said that the Taliban’s decision will have major repercussions beyond the Afghan border, as people from both sides frequently travel to each other’s country.
The World Health Organization has confirmed 18 polio cases in Afghanistan this year, all but two in the south of the country. That’s up from six cases in 2023. Afghanistan used a house-to-house vaccination strategy this June for the first time in five years, a tactic that helped to reach the majority of children targeted, according to WHO.
Health officials in Pakistan say they want the both sides to conduct anti-polio drives simultaneously.
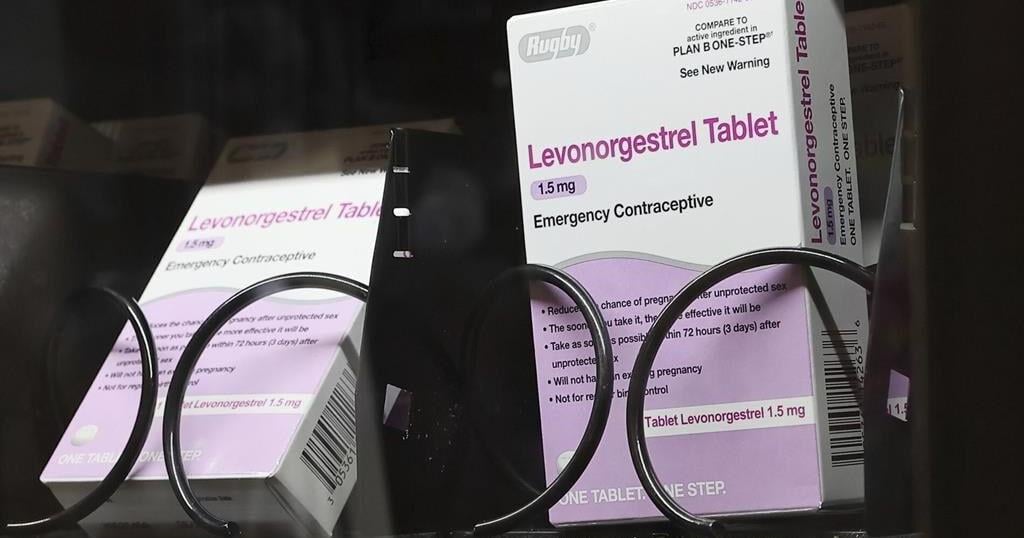
WASHINGTON (AP) — Millions of people with private health insurance would be able to pick up over-the-counter methods like condoms, the “morning after” pill and birth control pills for free under a new rule the White House proposed on Monday.
Right now, health insurers must cover the cost of prescribed contraception, including prescription birth control or even condoms that doctors have issued a prescription for. But the new rule would expand that coverage, allowing millions of people on private health insurance to pick up free condoms, birth control pills, or “morning after” pills from local storefronts without a prescription.
The proposal comes days before Election Day, as Vice President Kamala Harris affixes her presidential campaign to a promise of expanding women’s health care access in the wake of the U.S. Supreme Court’s decision to undo nationwide abortion rights two years ago. Harris has sought to craft a distinct contrast from her Republican challenger, Donald Trump, who appointed some of the judges who issued that ruling.
“The proposed rule we announce today would expand access to birth control at no additional cost for millions of consumers,” Health and Human Services Secretary Xavier Becerra said in a statement. “Bottom line: women should have control over their personal health care decisions. And issuers and providers have an obligation to comply with the law.”
The emergency contraceptives that people on private insurance would be able to access without costs include levonorgestrel, a pill that needs to be taken immediately after sex to prevent pregnancy and is more commonly known by the brand name “Plan B.”
Without a doctor’s prescription, women may pay as much as $50 for a pack of the pills. And women who delay buying the medication in order to get a doctor’s prescription could jeopardize the pill’s effectiveness, since it is most likely to prevent a pregnancy within 72 hours after sex.
If implemented, the new rule would also require insurers to fully bear the cost of the once-a-day Opill, a new over-the-counter birth control pill that the U.S. Food and Drug Administration approved last year. A one-month supply of the pills costs $20.
Federal mandates for private health insurance to cover contraceptive care were first introduced with the Affordable Care Act, which required plans to pick up the cost of FDA-approved birth control that had been prescribed by a doctor as a preventative service.
The proposed rule would not impact those on Medicaid, the insurance program for the poorest Americans. States are largely left to design their own rules around Medicaid coverage for contraception, and few cover over-the-counter methods like Plan B or condoms.