As COVID cases rise, Hamilton is missing a key tool used by the province as an early warning system.
Wastewater surveillance has been called the “canary in the coal mine” by Health Minister Christine Elliott and a closely monitored “key indicator” by chief medical officer of health Dr. Kieran Moore.
Wastewater data updated daily by the Ontario COVID-19 Science Advisory Table shows the virus is increasing across the province, including in Central West, which is Hamilton, Brant, Haldimand, Norfolk, Niagara, Waterloo and Wellington-Dufferin-Guelph.
But Hamilton public health doesn’t understand local wastewater surveillance data by it’s own admission. The department pulled its associate medical officer of health off of the project when resources became overwhelmed during the Omicron wave.
The reliability of wastewater surveillance has repeatedly been called into question by medical officer of health Dr. Elizabeth Richardson.
“Wastewater data continues to be under evaluation,” she said in a statement last week after making similar remarks to the board of health and at a city briefing.
She also blamed a lack of guidance from the province for the city’s reluctance to incorporate wastewater as a monitoring tool.
“There is no provincial guidance on its use for surveillance or disease control,” she said.
But Coun. John-Paul Danko questioned, “What guidance are we looking for from the province?”
He pointed to Ontario’s $22-million investment in surveillance at more than 170 locations covering all public health units.
“The reliance on wastewater signal for COVID seems to be fairly substantial across the province,” Danko said at a board of health meeting on March 21.
He raised the importance of wastewater as the general public has no access to PCR testing, making other metrics significantly underestimated.
“I think there would be a concern then that we’re not actually verifying the prevalence of COVID in the community,” said Danko. “The viral signal in the wastewater is one method of verifying.”
In addition, he asked about public health’s long insistence that wastewater surveillance hasn’t worked in Hamilton. Data made public for the first time on March 11 appears to show wastewater has been providing early warning of cases, hospitalizations, intensive care unit (ICU) admissions and deaths.
“I’m just looking at this as a layperson but it seems to me that for Omicron they are quite closely aligned to date,” said Danko.
The surveillance has been called “remarkable” by the lead researcher of the team at the University of Ottawa that has been analyzing the data from the Woodward Avenue and Dundas treatment plants since July 2020. Robert Delatolla claims wastewater has been an early predictor of Hamilton hospitalizations for over 18 months now.
Delatolla said in recent weeks there has been effort to come to an understanding between researchers and Hamilton public health since The Spectator started publishing stories on the divide March 5.
Richardson said public health is working with the university and the Ministry of the Environment, Conservation and Parks “to understand the data overall” and how it functions as an early indicator.
In addition, she says public health has kept in contact with Moore’s office, “and our approach that we are taking here in Hamilton has been supported … by the chief medical officer of health.”
A statement from the Ministry of Health neither confirms nor denies support for Hamilton’s stance on wastewater, but makes clear the province is using it as a key metric.
“At this time, the Ministry of Health is using the wastewater surveillance data in conjunction with other public health and health system indicators … to monitor the current epidemiology of the COVID-19 pandemic in Ontario,” it said.
Dr. Bart Harvey was looking at how wastewater could be similarly used to monitor COVID in Hamilton, but the associate medical officer of health was pulled away during the fifth wave that started in December.
“The unprecedented surge in infections and outbreaks in high-risk settings led Hamilton Public Health Services to prioritize resources to reduce the transmission of COVID-19 and its impact on the community,” Richardson said. “Dr. Harvey’s time, as with all staff, was prioritized to support the most urgent areas of the response.”
Richardson said there was still engagement with the project over the Omicron wave but at a “lower level.” Now, she’s waiting for provincial guidance that isn’t expected until the fall.
That time lag is significant considering COVID is on the rise. Hamilton’s average daily cases and weekly rate per 100,000 population have been increasing since March 19.
Hospital staff self-isolating was up to 394 Monday compared to 292 just under one week ago. During that same time, COVID patients hospitalized increased to 82 from 49.
Outbreaks in high-risk settings are up to 15 after holding steady between five and 10 for more than one month.
The city reported two deaths since Wednesday to bring the toll to 528 — one was a senior age 80 or older and the other was in their 70s.
Some Ontario doctors have started offering a free shot that can protect babies from respiratory syncytial virus while Quebec will begin its immunization program next month.
The new shot called Nirsevimab gives babies antibodies that provide passive immunity to RSV, a major cause of serious lower respiratory tract infections for infants and seniors, which can cause bronchiolitis or pneumonia.
Ontario’s ministry of health says the shot is already available at some doctor’s offices in Ontario with the province’s remaining supply set to arrive by the end of the month.
Quebec will begin administering the shots on Nov. 4 to babies born in hospitals and delivery centers.
Parents in Quebec with babies under six months or those who are older but more vulnerable to infection can also book immunization appointments online.
The injection will be available in Nunavut and Yukon this fall and winter, though administration start dates have not yet been announced.
This report by The Canadian Press was first published Oct. 21, 2024.
-With files from Nicole Ireland
Canadian Press health coverage receives support through a partnership with the Canadian Medical Association. CP is solely responsible for this content.
ISLAMABAD (AP) — Polio cases are rising ahead of a new vaccination campaign in Pakistan, where violence targeting health workers and the police protecting them has hampered years of efforts toward making the country polio-free.
Since January, health officials have confirmed 39 new polio cases in Pakistan, compared to only six last year, said Anwarul Haq of the National Emergency Operation Center for Polio Eradication.
The new nationwide drive starts Oct. 28 with the aim to vaccinate at least 32 million children. “The whole purpose of these campaigns is to achieve the target of making Pakistan a polio-free state,” he said.
Pakistan regularly launches campaigns against polio despite attacks on the workers and police assigned to the inoculation drives. Militants falsely claim the vaccination campaigns are a Western conspiracy to sterilize children.
Most of the new polio cases were reported in the southwestern Balochistan and southern Sindh province, following by Khyber Pakhtunkhwa province and eastern Punjab province.
The locations are worrying authorities since previous cases were from the restive northwest bordering Afghanistan, where the Taliban government in September suddenly stopped a door-to-door vaccination campaign.
Afghanistan and Pakistan are the two countries in which the spread of the potentially fatal, paralyzing disease has never been stopped. Authorities in Pakistan have said that the Taliban’s decision will have major repercussions beyond the Afghan border, as people from both sides frequently travel to each other’s country.
The World Health Organization has confirmed 18 polio cases in Afghanistan this year, all but two in the south of the country. That’s up from six cases in 2023. Afghanistan used a house-to-house vaccination strategy this June for the first time in five years, a tactic that helped to reach the majority of children targeted, according to WHO.
Health officials in Pakistan say they want the both sides to conduct anti-polio drives simultaneously.
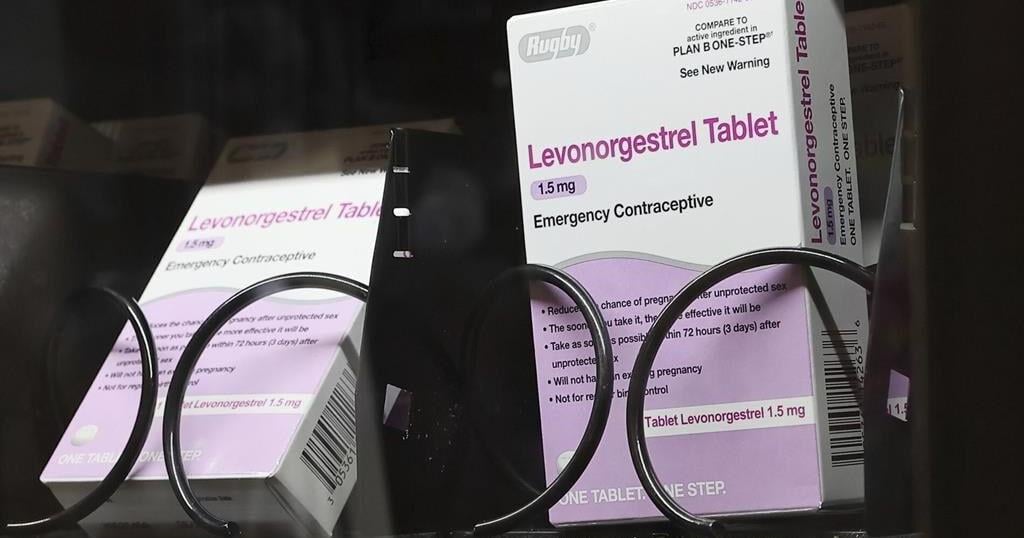
WASHINGTON (AP) — Millions of people with private health insurance would be able to pick up over-the-counter methods like condoms, the “morning after” pill and birth control pills for free under a new rule the White House proposed on Monday.
Right now, health insurers must cover the cost of prescribed contraception, including prescription birth control or even condoms that doctors have issued a prescription for. But the new rule would expand that coverage, allowing millions of people on private health insurance to pick up free condoms, birth control pills, or “morning after” pills from local storefronts without a prescription.
The proposal comes days before Election Day, as Vice President Kamala Harris affixes her presidential campaign to a promise of expanding women’s health care access in the wake of the U.S. Supreme Court’s decision to undo nationwide abortion rights two years ago. Harris has sought to craft a distinct contrast from her Republican challenger, Donald Trump, who appointed some of the judges who issued that ruling.
“The proposed rule we announce today would expand access to birth control at no additional cost for millions of consumers,” Health and Human Services Secretary Xavier Becerra said in a statement. “Bottom line: women should have control over their personal health care decisions. And issuers and providers have an obligation to comply with the law.”
The emergency contraceptives that people on private insurance would be able to access without costs include levonorgestrel, a pill that needs to be taken immediately after sex to prevent pregnancy and is more commonly known by the brand name “Plan B.”
Without a doctor’s prescription, women may pay as much as $50 for a pack of the pills. And women who delay buying the medication in order to get a doctor’s prescription could jeopardize the pill’s effectiveness, since it is most likely to prevent a pregnancy within 72 hours after sex.
If implemented, the new rule would also require insurers to fully bear the cost of the once-a-day Opill, a new over-the-counter birth control pill that the U.S. Food and Drug Administration approved last year. A one-month supply of the pills costs $20.
Federal mandates for private health insurance to cover contraceptive care were first introduced with the Affordable Care Act, which required plans to pick up the cost of FDA-approved birth control that had been prescribed by a doctor as a preventative service.
The proposed rule would not impact those on Medicaid, the insurance program for the poorest Americans. States are largely left to design their own rules around Medicaid coverage for contraception, and few cover over-the-counter methods like Plan B or condoms.