Cohorts of younger adults (n=300) and older adults (n=300) in Phase 2 study fully enrolled
Cohorts of older adults (ages 56-70, n=30) and elderlyadults (ages 71 and above, n=30) in NIH-led Phase 1 study completed enrollment; results expected to be published once available
Pivotal Phase 3 study expected to begin in July; manufacture of vaccine required to start Phase 3 study completed
Moderna, Inc., (Nasdaq: MRNA) a clinical stage biotechnology company pioneering messenger RNA (mRNA) therapeutics and vaccines to create a new generation of transformative medicines for patients, today announced that it has completed enrollment for both cohorts of the Phase 2 study of its vaccine candidate (mRNA-1273) against COVID-19. mRNA-1273 is Moderna’s second mRNA vaccine for an infectious disease to complete enrollment of a Phase 2 study, following the Company’s CMV Phase 2 study, which was fully enrolled on March 3, 2020.
On June 11, 13 days after the first participant was dosed, the Company announced that the cohort of healthy younger adults ages 18-55 (n=300) and the sentinel group of older adults ages 55 years and above (n=50) in the Phase 2 study of mRNA-1273 was complete. After reviewing the safety data from the sentinel cohort of older adults, on June 25, the Data and Safety Monitoring Committee of the study recommended Moderna to proceed with enrollment for the remainder of the Phase 2 study. The cohort of older adults (n=300) has now been fully enrolled. This Phase 2 placebo-controlled, dose-confirmation study is evaluating the safety, reactogenicity and immunogenicity of two vaccinations of mRNA-1273 given 28 days apart. Each participant is receiving placebo, a 50 µg or a 100 µg dose at both vaccinations.
The Company also announced that the cohorts of older adults (ages 56-70, n=30) and elderly adults (ages 71 and above, n=30) in NIH-led Phase 1 study have completed enrollment. Results are expected to be published once available.
“I would like to thank the healthy volunteer participants, our partners at clinical trial sites and the dedicated Moderna team for their support in completing enrollment of the Phase 2 study of mRNA-1273, our vaccine candidate against COVID-19,” said Tal Zaks, M.D., Ph.D., Chief Medical Officer at Moderna. “We are committed to helping address this ongoing public health emergency and continue to focus on our Phase 3 study, which remains on track to start in July, less than seven months from the sequencing of the virus.”
Moderna has finalized the Phase 3 study protocol based on feedback from the U.S. Food and Drug Administration (FDA). The randomized, 1:1 placebo-controlled trial is expected to include approximately 30,000 participants at the 100 µg dose level in the U.S. and is expected to be conducted in collaboration with NIAID, subject to regulatory approval. Moderna has completed manufacture of vaccine required to start the Phase 3 study. With the Phase 3 dose at 100 µg, the Company remains on track to be able to deliver approximately 500 million doses per year, and possibly up to 1 billion doses per year, beginning in 2021 from the Company’s internal U.S. manufacturing site and strategic collaboration with Lonza. In addition, Moderna recently announced a collaboration with Catalent for large-scale, commercial fill-finish manufacturing of mRNA-1273 at Catalent’s biologics facility in Indiana.
About mRNA-1273
mRNA-1273 is an mRNA vaccine against COVID-19 encoding for a prefusion stabilized form of the Spike (S) protein, which was selected by Moderna in collaboration with investigators from the VRC. The first clinical batch, which was funded by the Coalition for Epidemic Preparedness Innovations, was completed on February 7, 2020 and underwent analytical testing; it was shipped to NIH on February 24, 42 days from sequence selection. The first participant in the NIAID-led Phase 1 study of mRNA-1273 was dosed on March 16, 63 days from sequence selection to Phase 1 study dosing. On May 12, the FDA granted mRNA-1273 Fast Track designation.
About Moderna’s Prophylactic Vaccines Modality
Moderna scientists designed the company’s prophylactic vaccines modality to prevent infectious diseases. More than 1,600 participants have been enrolled in Moderna’s infectious disease vaccine clinical studies under health authorities in the U.S., Europe and Australia. Clinical data demonstrate that Moderna’s proprietary vaccine technology has been generally well-tolerated and can elicit durable immune responses to viral antigens. Based on clinical experience across Phase 1 studies, the company designated prophylactic vaccines a core modality and is working to accelerate the development of its vaccine pipeline.
The potential advantages of an mRNA approach to prophylactic vaccines include the ability to combine multiple mRNAs into a single vaccine, rapid discovery to respond to emerging pandemic threats and manufacturing agility derived from the platform nature of mRNA vaccine design and production. Moderna has built a fully integrated manufacturing plant which enables the promise of the technology platform.
Respiratory syncytial virus (RSV) vaccine for older adults (mRNA-1777 and mRNA-1172 or V172 with Merck)
RSV vaccine for young children (mRNA-1345)
Human metapneumovirus (hMPV) and parainfluenza virus type 3 (PIV3) vaccine (mRNA-1653)
COVID-19 vaccine (mRNA-1273)
Influenza H7N9 (mRNA-1851)
Vaccines against infections transmitted from mother to baby
Cytomegalovirus (CMV) vaccine (mRNA-1647)
Zika vaccine (mRNA-1893 with BARDA)
Vaccines against highly prevalent viral infections
Epstein-Barr virus (EBV) vaccine (mRNA-1189)
To date, Moderna has demonstrated positive Phase 1 data readouts for seven prophylactic vaccines (H10N8, H7N9, RSV, chikungunya virus, hMPV/PIV3, CMV and Zika). Moderna’s CMV vaccine is currently in a Phase 2 dose-confirmation study. Moderna’s investigational Zika vaccine (mRNA-1893), currently in a Phase 1 study, was granted FDA Fast Track designation in August 2019.
About Moderna
Moderna is advancing messenger RNA (mRNA) science to create a new class of transformative medicines for patients. mRNA medicines are designed to direct the body’s cells to produce intracellular, membrane or secreted proteins that can have a therapeutic or preventive benefit and have the potential to address a broad spectrum of diseases. The company’s platform builds on continuous advances in basic and applied mRNA science, delivery technology and manufacturing, providing Moderna the capability to pursue in parallel a robust pipeline of new development candidates. Moderna is developing therapeutics and vaccines for infectious diseases, immuno-oncology, rare diseases and cardiovascular diseases, independently and with strategic collaborators.
Headquartered in Cambridge, Mass., Moderna currently has strategic alliances for development programs with AstraZeneca PLC and Merck & Co., Inc., as well as the Defense Advanced Research Projects Agency (DARPA), an agency of the U.S. Department of Defense, and the Biomedical Advanced Research and Development Authority (BARDA), a division of the Office of the Assistant Secretary for Preparedness and Response (ASPR) within the U.S. Department of Health and Human Services (HHS). Moderna has been ranked in the top ten of Science’s list of top biopharma industry employers for the past five years. To learn more, visit www.modernatx.com.
Forward Looking Statements
This press release contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995, as amended, including regarding the Company’s development of a potential vaccine against the novel coronavirus, the parameters and timing of the Phase 2 and planned Phase 3 studies of mRNA-1273, and the Company’s potential manufacturing capabilities and projected vaccine dose production. In some cases, forward-looking statements can be identified by terminology such as “will,” “may,” “should,” “could”, “expects,” “intends,” “plans,” “aims,” “anticipates,” “believes,” “estimates,” “predicts,” “potential,” “continue,” or the negative of these terms or other comparable terminology, although not all forward-looking statements contain these words. The forward-looking statements in this press release are neither promises nor guarantees, and you should not place undue reliance on these forward-looking statements because they involve known and unknown risks, uncertainties, and other factors, many of which are beyond Moderna’s control and which could cause actual results to differ materially from those expressed or implied by these forward-looking statements. These risks, uncertainties, and other factors include, among others: the fact that there has never been a commercial product utilizing mRNA technology approved for use; the fact that the rapid response technology in use by Moderna is still being developed and implemented; the fact that the safety and efficacy of mRNA-1273 has not yet been established; potential adverse impacts due to the global COVID-19 pandemic such as delays in regulatory review, manufacturing and clinical trials, supply chain interruptions, adverse effects on healthcare systems and disruption of the global economy; and those other risks and uncertainties described under the heading “Risk Factors” in Moderna’s most recent Quarterly Report on Form 10-Q filed with the U.S. Securities and Exchange Commission (SEC) and in subsequent filings made by Moderna with the SEC, which are available on the SEC’s website at www.sec.gov. Except as required by law, Moderna disclaims any intention or responsibility for updating or revising any forward-looking statements contained in this press release in the event of new information, future developments or otherwise. These forward-looking statements are based on Moderna’s current expectations and speak only as of the date hereof.
LONDON (AP) — Most people have accumulated a pile of data — selfies, emails, videos and more — on their social media and digital accounts over their lifetimes. What happens to it when we die?
It’s wise to draft a will spelling out who inherits your physical assets after you’re gone, but don’t forget to take care of your digital estate too. Friends and family might treasure files and posts you’ve left behind, but they could get lost in digital purgatory after you pass away unless you take some simple steps.
Here’s how you can prepare your digital life for your survivors:
Apple
The iPhone maker lets you nominate a “ legacy contact ” who can access your Apple account’s data after you die. The company says it’s a secure way to give trusted people access to photos, files and messages. To set it up you’ll need an Apple device with a fairly recent operating system — iPhones and iPads need iOS or iPadOS 15.2 and MacBooks needs macOS Monterey 12.1.
For iPhones, go to settings, tap Sign-in & Security and then Legacy Contact. You can name one or more people, and they don’t need an Apple ID or device.
You’ll have to share an access key with your contact. It can be a digital version sent electronically, or you can print a copy or save it as a screenshot or PDF.
Take note that there are some types of files you won’t be able to pass on — including digital rights-protected music, movies and passwords stored in Apple’s password manager. Legacy contacts can only access a deceased user’s account for three years before Apple deletes the account.
Google
Google takes a different approach with its Inactive Account Manager, which allows you to share your data with someone if it notices that you’ve stopped using your account.
When setting it up, you need to decide how long Google should wait — from three to 18 months — before considering your account inactive. Once that time is up, Google can notify up to 10 people.
You can write a message informing them you’ve stopped using the account, and, optionally, include a link to download your data. You can choose what types of data they can access — including emails, photos, calendar entries and YouTube videos.
There’s also an option to automatically delete your account after three months of inactivity, so your contacts will have to download any data before that deadline.
Facebook and Instagram
Some social media platforms can preserve accounts for people who have died so that friends and family can honor their memories.
When users of Facebook or Instagram die, parent company Meta says it can memorialize the account if it gets a “valid request” from a friend or family member. Requests can be submitted through an online form.
The social media company strongly recommends Facebook users add a legacy contact to look after their memorial accounts. Legacy contacts can do things like respond to new friend requests and update pinned posts, but they can’t read private messages or remove or alter previous posts. You can only choose one person, who also has to have a Facebook account.
You can also ask Facebook or Instagram to delete a deceased user’s account if you’re a close family member or an executor. You’ll need to send in documents like a death certificate.
TikTok
The video-sharing platform says that if a user has died, people can submit a request to memorialize the account through the settings menu. Go to the Report a Problem section, then Account and profile, then Manage account, where you can report a deceased user.
Once an account has been memorialized, it will be labeled “Remembering.” No one will be able to log into the account, which prevents anyone from editing the profile or using the account to post new content or send messages.
X
It’s not possible to nominate a legacy contact on Elon Musk’s social media site. But family members or an authorized person can submit a request to deactivate a deceased user’s account.
Passwords
Besides the major online services, you’ll probably have dozens if not hundreds of other digital accounts that your survivors might need to access. You could just write all your login credentials down in a notebook and put it somewhere safe. But making a physical copy presents its own vulnerabilities. What if you lose track of it? What if someone finds it?
Instead, consider a password manager that has an emergency access feature. Password managers are digital vaults that you can use to store all your credentials. Some, like Keeper,Bitwarden and NordPass, allow users to nominate one or more trusted contacts who can access their keys in case of an emergency such as a death.
But there are a few catches: Those contacts also need to use the same password manager and you might have to pay for the service.
___
Is there a tech challenge you need help figuring out? Write to us at onetechtip@ap.org with your questions.
The Canadian Paediatric Society says doctors should regularly screen children for reading difficulties and dyslexia, calling low literacy a “serious public health concern” that can increase the risk of other problems including anxiety, low self-esteem and behavioural issues, with lifelong consequences.
New guidance issued Wednesday says family doctors, nurses, pediatricians and other medical professionals who care for school-aged kids are in a unique position to help struggling readers access educational and specialty supports, noting that identifying problems early couldhelp kids sooner — when it’s more effective — as well as reveal other possible learning or developmental issues.
The 10 recommendations include regular screening for kids aged four to seven, especially if they belong to groups at higher risk of low literacy, including newcomers to Canada, racialized Canadians and Indigenous Peoples. The society says this can be done in a two-to-three-minute office-based assessment.
Other tips encourage doctors to look for conditions often seen among poor readers such as attention-deficit hyperactivity disorder; to advocate for early literacy training for pediatric and family medicine residents; to liaise with schools on behalf of families seeking help; and to push provincial and territorial education ministries to integrate evidence-based phonics instruction into curriculums, starting in kindergarten.
Dr. Scott McLeod, one of the authors and chair of the society’s mental health and developmental disabilities committee, said a key goal is to catch kids who may be falling through the cracks and to better connect families to resources, including quicker targeted help from schools.
“Collaboration in this area is so key because we need to move away from the silos of: everything educational must exist within the educational portfolio,” McLeod said in an interview from Calgary, where he is a developmental pediatrician at Alberta Children’s Hospital.
“Reading, yes, it’s education, but it’s also health because we know that literacy impacts health. So I think that a statement like this opens the window to say: Yes, parents can come to their health-care provider to get advice, get recommendations, hopefully start a collaboration with school teachers.”
McLeod noted that pediatricians already look for signs of low literacy in young children by way of a commonly used tool known as the Rourke Baby Record, which offers a checklist of key topics, such as nutrition and developmental benchmarks, to cover in a well-child appointment.
But he said questions about reading could be “a standing item” in checkups and he hoped the society’s statement to medical professionals who care for children “enhances their confidence in being a strong advocate for the child” while spurring partnerships with others involved in a child’s life such as teachers and psychologists.
The guidance said pediatricians also play a key role in detecting and monitoring conditions that often coexist with difficulty reading such as attention-deficit hyperactivity disorder, but McLeod noted that getting such specific diagnoses typically involves a referral to a specialist, during which time a child continues to struggle.
He also acknowledged that some schools can be slow to act without a specific diagnosis from a specialist, and even then a child may end up on a wait list for school interventions.
“Evidence-based reading instruction shouldn’t have to wait for some of that access to specialized assessments to occur,” he said.
“My hope is that (by) having an existing statement or document written by the Canadian Paediatric Society … we’re able to skip a few steps or have some of the early interventions present,” he said.
McLeod added that obtaining specific assessments from medical specialists is “definitely beneficial and advantageous” to know where a child is at, “but having that sort of clear, thorough assessment shouldn’t be a barrier to intervention starting.”
McLeod said the society was partly spurred to act by 2022’s “Right to Read Inquiry Report” from the Ontario Human Rights Commission, which made 157 recommendations to address inequities related to reading instruction in that province.
He called the new guidelines “a big reminder” to pediatric providers, family doctors, school teachers and psychologists of the importance of literacy.
“Early identification of reading difficulty can truly change the trajectory of a child’s life.”
This report by The Canadian Press was first published Oct. 23, 2024.
LONDON (AP) — Britain’s drug regulator approved the Alzheimer’s drug Kisunla on Wednesday, but the government won’t be paying for it after an independent watchdog agency said the treatment isn’t worth the cost to taxpayers.
It is the second Alzheimer’s drug to receive such a mixed reception within months. In August, the U.K. regulator authorized Leqembi while the same watchdog agency issued draft guidance recommending against its purchase for the National Health Service.
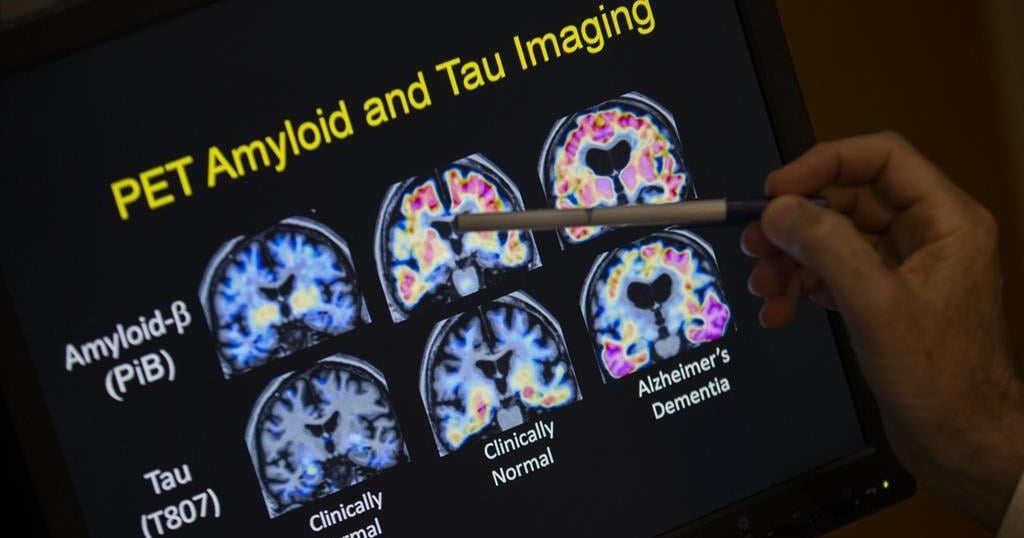
In a statement on Wednesday, Britain’s Medicines and Healthcare regulatory Agency said Kisunla “showed some evidence of efficacy in slowing (Alzheimer’s) progression” and approved its use to treat people in the early stages of the brain-robbing disease. Kisunla, also known as donanemab, works by removing a sticky protein from the brain believed to cause Alzheimer’s disease.
Meanwhile, the National Institute for Health and Care Excellence, or NICE, said more evidence was needed to prove Kisunla’s worth — the drug’s maker, Eli Lilly, says a year’s worth of treatment is $32,000. The U.S. Food and Drug Administration authorized Kisunla in July. The roll-out of its competitor drug Leqembi has been slowed in the U.S. by spotty insurance coverage, logistical hurdles and financial worries.
NICE said that the cost of administering Kisunla, which requires regular intravenous infusions and rigorous monitoring for potentially severe side effects including brain swelling or bleeding, “means it cannot currently be considered good value for the taxpayer.”
Experts at NICE said they “recognized the importance of new treatment options” for Alzheimer’s and asked Eli Lilly and the National Health Service “to provide additional information to address areas of uncertainty in the evidence.”
Under Britain’s health care system, most people receive free health care paid for by the government, but they could get Kisunla if they were to pay for it privately.
“People living with dementia and their loved ones will undoubtedly be disappointed by the decision not to fund this new treatment,” said Tara Spires-Jones, director of the Centre for Discovery Brain Sciences at the University of Edinburgh. “The good news that new treatments can slow disease even a small amount is helpful,” she said in a statement, adding that new research would ultimately bring safer and more effective treatments.
Fiona Carragher, chief policy and research officer at the Alzheimer’s Society, said the decision by NICE was “disheartening,” but noted there were about 20 Alzheimer’s drugs being tested in advanced studies, predicting that more drugs would be submitted for approval within years.
“In other diseases like cancer, treatments have become more effective, safer and cheaper over time,” she said. “ We hope to see similar progress in dementia.”
___
The Associated Press Health and Science Department receives support from the Howard Hughes Medical Institute’s Science and Educational Media Group. The AP is solely responsible for all content.