White Coat Black Art26:29Preventing ovarian cancer
Lindsay Mazepa had never heard of opportunistic salpingectomy.
But when Mazepa was discussing her upcoming C-section for the birth of her twins, her obstetrician-gynecologist suggested the procedure instead of the tubal ligation for family planning they were already considering.
The 43-year-old mom of three in Port Coquitlam, B.C., says her doctor explained at the time that the procedure would “significantly decrease” any chances of ovarian cancer in the future.
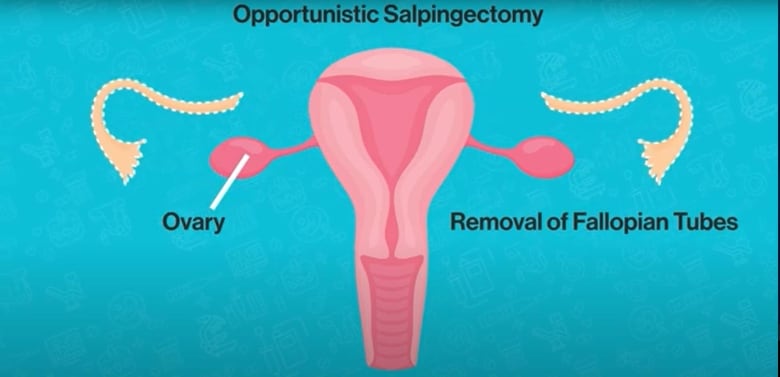
Opportunistic salpingectomy is the removal of the fallopian tubes in an average-risk woman who is done having children and is already undergoing a gynecological surgery, such as a C-section or surgery for endometriosis. The ovaries are left intact.
An illustration shows the ovaries and the removal of the fallopian tubes during an opportunistic salpingectomy. (Screenshot/Gynecologic Cancer Initiative)
In a tubal ligation performed solely as a method of permanent birth control, the fallopian tubes are usually cut, clamped or sealed, but not removed.
“Considering I was already having the surgery and that she had mentioned that there would be literally only a 10-minute extra procedure, the recovery period would be exactly the same, that was really all I needed to hear that it would decrease my risk of [ovarian] cancer in the future,” said Mazepa, a neurodiagnostic technologist, told White Coat, Black Art.
The procedure is considered to be one of the few ways to reduce the risk of ovarian cancer, which doctors say can be difficult to detect. There is no effective screening test for the disease.
About one in 75 Canadian women will be diagnosed with ovarian cancer, according to Ovarian Cancer Canada.
Early research has shown that an opportunistic salpingectomy can help reduce the risk of ovarian cancer.
“We now recognize that the majority of ovarian cancers are a specific subtype called high-grade serous carcinoma and the majority of these cancers actually arise in the fallopian tube, not the ovary,” said Dr. Janice Kwon, a gynecologic oncologist with Vancouver General Hospital and BC Cancer, and vice-head of University of British Columbia’s obstetrics and gynecology department.
Dr. Janice Kwon, a gynecologic oncologist with Vancouver General Hospital and BC Cancer, says ovarian cancer is something that she sees almost on a daily basis. (Submitted by Janice Kwon)
Opportunistic salpingectomy has been done in Canada for more than a decade on women who are done having children and are already undergoing a gynecological surgery.
B.C. has led the country in terms of the number of opportunistic salpingectomies perfomed.
Preliminary data analyzed by University of British Columbia obstetrics and gynecology associate professor Gillian Hanley and colleagues shows that uptake has grown since their previous look at data from all provinces except Quebec from 2011 to 2016.
University of British Columbia associate professor Gillian Hanley says opportunistic salpingectomies rates are increasing, but there’s ‘still definitely room for improvement.’ (Submitted by Gillian Hanley)
“It does look like rates are increasing in other provinces, which is great,” Hanley told White Coat, Black Art. “But there is still definitely room for improvement.”
Previously, rates were very low, less than one in 10, in several Maritime provinces. Now in Nova Scotia, Hanley said nearly half of tubal sterilizations are opportunistic salpingectomy.
Hanley said she would like to see higher uptake in P.E.I., Newfoundland and Labrador, Ontario and Manitoba, saying opportunities to save lives are being missed.
A Canadian discovery
Dr. Dianne Miller, associate professor emerita at UBC’s department of obstetrics and gynecology, was the first to develop and name opportunistic salpingectomy as an ovarian cancer prevention strategy.
In 2010, an education campaign rolled out in B.C. to explain the benefits of opportunistic salpingectomy.
Prior to 2010, Kwon says “a very small proportion of women” had their fallopian tubes removed, sometimes to prevent an unplanned pregnancy or during a hysterectomy for non-cancerous reasons, such as abnormal bleeding or endometriosis.
Since then, several organizations in Canada and elsewhere have come out with recommendations for those with average risk for ovarian cancer to consider having an opportunistic salpingectomy.
Most recently in February, the global non-profit Ovarian Cancer Research Alliance and the Society of Gynecologic Oncology in the U.S. released a joint statement encouraging women undergoing pelvic surgeries to also have their fallopian tubes removed.
Hanley said B.C.’s approach to opportunistic salpingectomy is recommended in nine other countries. Researchers in The Netherlands found when health professionals offered the procedure to patients, nearly 96 per cent chose to proceed.
WATCH | Why specialists recommend doctors talk to patients about the surgery: [embedded content]
The procedure takes less than 15 minutes and is “very, very safe,” said Dr. Raz Moola, an obstetrician-gynecologist based out of Kootenay Lake Hospital. He routinely performs the surgery, but said he’s up front with his patients about what it can and can’t do.
“It’s important from my perspective to be clear with the patients that this procedure is meant to ideally prevent something from happening but we don’t actually know that it will,” he said, adding that fallopian tube cancer is one of about 20 different types of ovarian cancer.
The potential to lower risk
Donna Pepin was diagnosed with ovarian cancer in 2006, which recurred a decade later.
Pepin remembers being at the 2010 event when gynecologists in B.C.encouraged average-risk women to get opportunistic salpingectomy.
“I remember at the time I felt so emotional because I thought you know the lives potentially that could be saved, the suffering that can be avoided. For me it was this really huge moment of understanding, especially having gone through my own journey with ovarian cancer.”
Pepin has taken part in clinical trials, done several rounds of chemo treatment and undergone surgery.
Donna Pepin, an ovarian cancer patient, says at this point there’s no way to prevent this disease aside from opportunistic salpingectomy. (Submitted by Donna Pepin)
For nine years she was healthy. But in 2016 she was diagnosed with low-grade serous ovarian cancer, a rare type.
The 65-year-old takes medication that has allowed her disease to remain stable.
The Ovarian Cancer Canada volunteer says it’s been exciting seeing the medical science community make progress in ovarian cancer prevention.
“As an ovarian cancer patient, all of our community would agree that this is amazing just to be able to stop it from happening because there is no pap test. There is no way to detect our disease. There’s no way to prevent it that we are aware of aside from this one, opportunistic salpingectomy.”
On top of that, other health conditions can cause the same symptoms as ovarian cancer, according to the Canadian Cancer Society’s website.
Also, Kwon says the majority of women are diagnosed with ovarian cancer at an advanced stage where the cancer has spread (also known as metastasized) to other parts of the body.
“This becomes difficult to treat and cure,” she said.
Since the education campaign for opportunistic salpingectomy only launched just over 10 years ago, it’s still early to say what the true benefits of this procedure are, Kwon says.
But she adds early research is “exciting news.”
Research from Hanley, Kwon and colleagues published in the peer-reviewed Journal of the American Medical Association last year found that opportunistic salpingectomy could help to reduce the number of ovarian cancer cases.
Ovarian cancer is something that I see almost on a daily basis … and any opportunity we have to prevent ovarian cancer is certainly worthwhile.– Janice Kwon
They found that the nearly 26,000 individuals who underwent opportunistic salpingectomy had significantly fewer serous and epithelial ovarian cancers than were expected, compared to the rate among the control group who had either only a hysterectomy or tubal ligation.
When they looked at high-grade serous cancers in particular, there wasn’t a single case found among those who had their fallopian tubes removed.
“Ovarian cancer is something that I see almost on a daily basis. I’ve treated hundreds of women with that illness and any opportunity we have to prevent ovarian cancer is certainly worthwhile,” Kwon said.
Patients who are older, don’t speak English, and don’t have a high school education are more likely to experience harm during a hospital stay in Canada, according to new research.
The Canadian Institute for Health Information measured preventableharmful events from 2023 to 2024, such as bed sores and medication errors,experienced by patients who received acute care in hospital.
The research published Thursday shows patients who don’t speak English or French are 30 per cent more likely to experience harm. Patients without a high school education are 20 per cent more likely to endure harm compared to those with higher education levels.
The report also found that patients 85 and older are five times more likely to experience harm during a hospital stay compared to those under 20.
“The goal of this report is to get folks thinking about equity as being a key dimension of the patient safety effort within a hospital,” says Dana Riley, an author of the report and a program lead on CIHI’s population health team.
When a health-care provider and a patient don’t speak the same language, that can result in the administration of a wrong test or procedure, research shows. Similarly, Riley says a lower level of education is associated with a lower level of health literacy, which can result in increased vulnerability to communication errors.
“It’s fairly costly to the patient and it’s costly to the system,” says Riley, noting the average hospital stay for a patient who experiences harm is four times more expensive than the cost of a hospital stay without a harmful event – $42,558 compared to $9,072.
“I think there are a variety of different reasons why we might start to think about patient safety, think about equity, as key interconnected dimensions of health-care quality,” says Riley.
The analysis doesn’t include data on racialized patients because Riley says pan-Canadian data was not available for their research. Data from Quebec and some mental health patients was also excluded due to differences in data collection.
Efforts to reduce patient injuries at one Ontario hospital network appears to have resulted in less harm. Patient falls at Mackenzie Health causing injury are down 40 per cent, pressure injuries have decreased 51 per cent, and central line-associated bloodstream infections, such as IV therapy, have been reduced 34 per cent.
The hospital created a “zero harm” plan in 2019 to reduce errors after a hospital survey revealed low safety scores. They integrated principles used in aviation and nuclear industries, which prioritize safety in complex high-risk environments.
“The premise is first driven by a cultural shift where people feel comfortable actually calling out these events,” says Mackenzie Health President and Chief Executive Officer Altaf Stationwala.
They introduced harm reduction training and daily meetings to discuss risks in the hospital. Mackenzie partnered with virtual interpreters that speak 240 languages and understand medical jargon. Geriatric care nurses serve the nearly 70 per cent of patients over the age of 75, and staff are encouraged to communicate as frequently as possible, and in plain language, says Stationwala.
“What we do in health care is we take control away from patients and families, and what we know is we need to empower patients and families and that ultimately results in better health care.”
This report by The Canadian Press was first published Oct. 17, 2024.
Canadian Press health coverage receives support through a partnership with the Canadian Medical Association. CP is solely responsible for this content.
CALGARY – Alberta’s health minister says a new agency responsible for primary health care should be up and running by next month.
Adriana LaGrange says Primary Care Alberta will work to improve Albertans’ access to primary care providers like family doctors or nurse practitioners, create new models of primary care and increase access to after-hours care through virtual means.
Her announcement comes as the provincial government continues to divide Alberta Health Services into four new agencies.
LaGrange says Alberta Health Services hasn’t been able to focus on primary health care, and has been missing system oversight.
The Alberta government’s dismantling of the health agency is expected to include two more organizations responsible for hospital care and continuing care.
Another new agency, Recovery Alberta, recently took over the mental health and addictions portfolio of Alberta Health Services.
This report by The Canadian Press was first published Oct. 15, 2024.
Rana Van Tuyl was about 12 weeks pregnant when she got devastating news at her ultrasound appointment in December 2020.
Her fetus’s heartbeat had stopped.
“We were both shattered,” says Van Tuyl, who lives in Nanaimo, B.C., with her partner. Her doctor said she could surgically or medically pass the pregnancy and she chose the medical option, a combination of two drugs taken at home.
“That was the last I heard from our maternity physician, with no further followup,” she says.
But complications followed. She bled for a month and required a surgical procedure to remove pregnancy tissue her body had retained.
Looking back, Van Tuyl says she wishes she had followup care and mental health support as the couple grieved.
Her story is not an anomaly. Miscarriages affect one in five pregnancies in Canada, yet there is often a disconnect between the medical view of early pregnancy loss as something that is easily managed and the reality of the patients’ own traumatizing experiences, according to a paper published Tuesday in the Canadian Medical Association Journal.
An accompanying editorial says it’s time to invest in early pregnancy assessment clinics that can provide proper care during and after a miscarriage, which can have devastating effects.
The editorial and a review of medical literature on early pregnancy loss say patients seeking help in emergency departments often receive “suboptimal” care. Non-critical miscarriage cases drop to the bottom of the triage list, resulting in longer wait times that make patients feel like they are “wasting” health-care providers’ time. Many of those patients are discharged without a followup plan, the editorial says.
But not all miscarriages need to be treated in the emergency room, says Dr. Modupe Tunde-Byass, one of the authors of the literature review and an obstetrician/gynecologist at Toronto’s North York General Hospital.
She says patients should be referred to early pregnancy assessment clinics, which provide compassionate care that accounts for the psychological impact of pregnancy loss – including grief, guilt, anxiety and post-traumatic stress.
But while North York General Hospital and a patchwork of other health-care providers in the country have clinics dedicated to miscarriage care, Tunde-Byass says that’s not widely adopted – and it should be.
She’s been thinking about this gap in the Canadian health-care system for a long time, ever since her medical training almost four decades ago in the United Kingdom, where she says early pregnancy assessment centres are common.
“One of the things that we did at North York was to have a clinic to provide care for our patients, and also to try to bridge that gap,” says Tunde-Byass.
Provincial agency Health Quality Ontario acknowledged in 2019 the need for these services in a list of ways to better manage early pregnancy complications and loss.
“Five years on, little if any progress has been made toward achieving this goal,” Dr. Catherine Varner, an emergency physician, wrote in the CMAJ editorial. “Early pregnancy assessment services remain a pipe dream for many, especially in rural Canada.”
The quality standard released in Ontario did, however, prompt a registered nurse to apply for funding to open an early pregnancy assessment clinic at St. Joseph’s Healthcare Hamilton in 2021.
Jessica Desjardins says that after taking patient referrals from the hospital’s emergency room, the team quickly realized that they would need a bigger space and more people to provide care. The clinic now operates five days a week.
“We’ve been often hearing from our patients that early pregnancy loss and experiencing early pregnancy complications is a really confusing, overwhelming, isolating time for them, and (it) often felt really difficult to know where to go for care and where to get comprehensive, well-rounded care,” she says.
At the Hamilton clinic, Desjardins says patients are brought into a quiet area to talk and make decisions with providers – “not only (from) a physical perspective, but also keeping in mind the psychosocial piece that comes along with loss and the grief that’s a piece of that.”
Ashley Hilliard says attending an early pregnancy assessment clinic at The Ottawa Hospital was the “best case scenario” after the worst case scenario.
In 2020, she was about eight weeks pregnant when her fetus died and she hemorrhaged after taking medication to pass the pregnancy at home.
Shortly after Hilliard was rushed to the emergency room, she was assigned an OB-GYN at an early pregnancy assessment clinic who directed and monitored her care, calling her with blood test results and sending her for ultrasounds when bleeding and cramping persisted.
“That was super helpful to have somebody to go through just that, somebody who does this all the time,” says Hilliard.
“It was really validating.”
This report by The Canadian Press was first published Oct. 15, 2024.
Canadian Press health coverage receives support through a partnership with the Canadian Medical Association. CP is solely responsible for this content.