With the case toll rising fast, reaching nearly 10,000 on January 31, and face masks flying off store shelves, it’s no wonder questions — and fears — are swirling about 2019-nCoV, as the virus is known.
For most people in the US, though, there’s really no reason to worry. And while making sense of risks with a new, quick-spreading pathogen is tricky, infectious disease experts are helping us sort it out. Here are answers to your most burning questions about the new coronavirus and its risks.
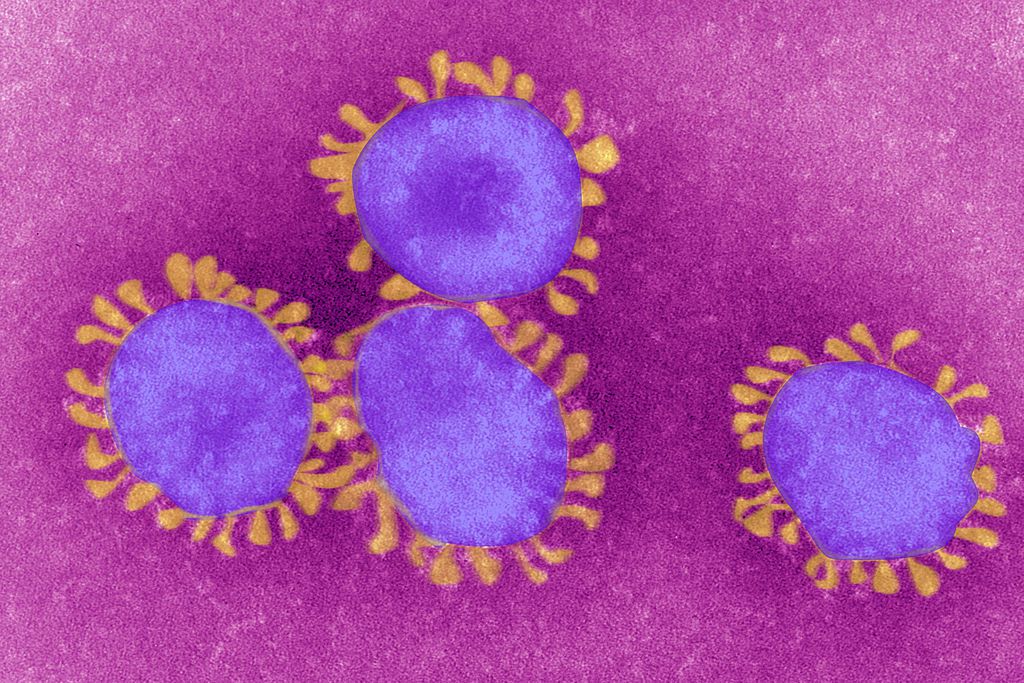
Universal Images Group via Getty
Coronaviruses are a large family of viruses that typically attack the respiratory system. The name comes from the Latin word corona, meaning crown, because of the spiky fringe that encircles these viruses. Most infect animals, such as bats, cats, and birds. Only seven, including 2019-nCoV, SARS, and MERS, are known to infect humans.
SARS is thought to have evolved from bats to civet cats to humans in China; MERS evolved from bats to camels to humans in the Middle East. No one knows where 2019-nCoV came from. For now, it is believed to have made the leap from animals in Wuhan, China, a city of 11 million, late last year. But researchers are still trying to suss out its precise origins.
As for symptoms: Two of the seven coronaviruses that infect humans, SARS and MERS, can cause severe pneumonia and even death in 10 and more than 30 percent of cases, respectively. But the others lead to milder symptoms, like a common cold. At the moment, we know 2019-nCoV can kill — but it’s not clear how often or how its fatality rate compares to SARS and MERS.
According to the Centers for Disease Control and Prevention, most patients right now start with a fever, cough, and shortness of breath. An early report, published in The Lancet, provided even more detailed information. It looked at a subset of the first 41 patients with confirmed 2019-nCoV in Wuhan. The most common symptoms were fever, cough, muscle pain, and fatigue; less common were headache, diarrhea, and coughing up mucus or blood. All had pneumonia and lung abnormalities on CT scans. As for the disease severity: 13 patients were admitted to an ICU, and six died. By January 22, most (68 percent) of the patients had been discharged from the hospital.
We don’t yet know how exactly 2019-nCoV spreads, but we do have a lot of data on how MERS, SARS, and other respiratory viruses move from person to person. And that’s mainly through exposure to dropletsfrom coughing or sneezing.
So when an infected person coughs or sneezes, they let out a spray, and if these droplets reach the nose, eyes, or mouth of another person, they can pass on the virus, said Jennifer Nuzzo, an infectious disease expert and senior scholar at the Johns Hopkins Center for Health Security. In rarer cases, a person might catch a respiratory disease indirectly, “via touching droplets on surfaces — and then touching mucosal membranes” in the mouth, eyes, and nose, she added. That’s why hand-washing is an important public health measure — all the time, and especially in an outbreak.
A tourist wearing a respiratory mask at the Trevi Fountain in downtown Rome on January 31, 2020. The Italian government declared a state of emergency to prevent the spread of the new coronavirus after two cases were confirmed in Rome.Filippo Monteforte/AFP via Getty Images
Both the CDC and the State Department have issued their highest-level travel alerts for China, advising Americans to avoid going to China for the moment. (These advisories are likely to change as the outbreak evolves, so keep checking them.)
And that’s not only because there’s a risk of catching this new virus. Right now, numerous airlines are canceling or scaling back flights to China, in part because of decreased demand. “I’m more concerned about the unpredictability of the [outbreak] response at this point,” said Nuzzo. “It would not be fun to go to China and get stuck there somehow. And coming back, you’ll be subject to additional screening.”
But people worried about travel should remember that these advisories focus on China, where the epidemic is currently playing out.
Of the 9,776 confirmed cases right now, 9,658 have been found in mainland China. That’s 99 percent. And more than half of those are in Hubei. “The risk of acquiring this infection outside of Hubei and, truly, outside of China is remarkably low,” said Isaac Bogoch, a professor at the University of Toronto who studies how air travel influences the dynamics outbreaks — including the new coronavirus infection.
Source: Johns Hopkins University Center for Systems Science and Engineering
People with the virus have been detected in other countries, which is the reason the WHO declared the outbreak a public health emergency. But to date, those have mainly been travelers from China. “We can count the number of people who never had exposure to Hubei or China who were infected by this virus on one or two hands,” Bogoch said. “So if people are traveling [anywhere outside of China,] your risk is close to zero percent.”
What if you have to travel and you’re seated near someone who is sick? Bogoch said that’s not even time to panic. “There has been some work looking into the risk of acquiring infectious diseases through air travel. The risk of acquiring a respiratory infection through air travel is still extraordinarily low.”
The risk does go up if you happen to be seated within two meters of a person with a respiratory infection. But even there, simple proximity doesn’t necessarily mean you’ll catch anything. Instead, the more infectious the person is, and the longer you sit near them, the higher your risk. If you’re not near the person for very long, or they’re not very infectious, the lower the risk.
People wear medical masks as a precaution against coronavirus, walking around New York, on January 30, 2020.Tayfun Coskun/Anadolu Agency via Getty Images
In the US, the risk to the public is currently deemed low. And just about every health expert Vox has spoken to has said there’s no good evidence to support the use of face masks for preventing disease in the general population.
Masks are only useful if you have a respiratory infection already and want to minimize the risk of spread to others, or if you’re working in a hospital and are in direct contact with people who have respiratory illnesses. (Plus, there are reports of runs on masks and other supplies health workers need to stay safe.)
That’s why the CDC advises against the use of masks for regular Americans. “The virus is not spreading in the general community,” Nancy Messonnier, director of the CDC’s National Center for Immunization and Respiratory Diseases, reasoned in a press briefing on January 30. But people are hoarding them anyway, and for the wrong reasons.
The best thing you can do to prevent all sorts of illness, said Messonnier, is “wash your hands, cover your cough, take care of yourself, and keep alert to the information that we’re providing.”
The best evidence we have that the virus can spread before a person has symptoms comes from Germany. There, four people are known to have the virus.
The outbreak was identified in Bavaria on January 27, when a German businessman was diagnosed. He had been in meetings with a female colleague who was visiting from Shanghai and had the virus but didn’t know it. The woman only began to feel symptoms — such as fever and a cough — after she left Germany, and days after meeting with the German businessman. This suggests she may have transmitted the virus to the man before knowing she was sick.
By January 28, three co-workers of the businessman were diagnosed with the virus, according to a New England Journal of Medicine case report. One had contact with the woman from Shanghai; the two others appear to have gotten the virus from the German businessman. “The fact that asymptomatic persons are potential sources of 2019-nCoV infection may warrant a reassessment of transmission dynamics of the current outbreak,” the study authors wrote.
But they also emphasized how mild the disease appeared to be among the German patients. And there’s the question of how much of a risk asymptomatic spread truly poses to public health. “Even if there have been cases of asymptomatic transmission of this infection, those will be typically rare cases, and with just about every other respiratory tract infection known to humankind, those are not the people who are driving an epidemic,” said Bogoch.
WHO Director-General Tedros Adhanom Ghebreyesus, right, with WHO Health Emergencies Program head Michael Ryan at a press conference following a WHO Emergency committee to discuss whether the new coronavirus constitutes an international health emergency, on January 30, 2020, in Geneva.Fabrice Coffrini/AFP via Getty Images
The WHO’s declaration of a “public health emergency of international concern,” or PHEIC, does not mean we are facing a deadly pandemic.
Instead, a PHEIC is a political tool the agency can use to draw attention to a serious disease threat. It’s meant to engage the global community in a coordinated outbreak response, galvanize resources, give countries guidance on how to react, and stop the disease from spreading further across borders.
The agency’s director general, Tedros Adhanom Ghebreyesus, was very clear that they sounded the alarm as a precautionary measure: The agency is concerned about the potential damage the virus could do in countries with weaker health systems, and called on the international community to help. He emphasized that the vast majority of cases are still in China, and that China has moved swiftly to get the outbreak under control.
If the disease continues to spread, however, it could turn into a pandemic: or a disease that spreads globally, with epidemics in multiple countries around the world. And that’s something health officials in the US and around the world are working to prevent. “We are preparing as if this is the next pandemic,” the CDC’s Messonnier said on January 31.
For now, the CDC and WHO are still calling this an outbreak. Very soon, health experts may determine that there are enough cases in China to call the outbreak an epidemic.
As for the question of deadliness, we don’t yet know how lethal this disease is or how easily it spreads. If you take the current number of deaths and divide it by the number of known cases, “the case fatality is 2 percent — and it’s gone down from 3 percent in the early days,” said University of Michigan’s Howard Markel, who studies outbreaks. “And if it goes really, really low, we’ll probably say — like we did in Mexico in 2009 with swine flu — that it’s something very similar, if not less deadly, than regular seasonal flu.”
So once more of these mild or asymptomatic cases are discovered, this virus could look a lot less scary.
“We live [with] and tolerate a whole lot of respiratory viruses,” said Nuzzo, “some of which are even more transmissible than the estimates people have come out with for this one — but they don’t make the headlines.” If the new coronavirus winds up looking less severe, she added, “we may be moving away from containing the virus as a goal to one of minimizing its spread.”
Two women wearing face masks on January 31, 2020, in Newcastle upon Tyne, England.Ian Forsyth/Getty Images
Some of the best research on that question comes from Bogoch and his colleagues. They’ve done great studies in the past couple of weeks on the cities most vulnerable to novel coronavirus infections. What’s the big takeaway?
It’s really East Asia and Southeast Asia that are most at risk. The researchers — from the University of Oxford, University of Toronto, and London School of Medicine and Tropical Hygiene — used 2019 data from the International Air Transport Association to find all the cities in China that received at least 100,000 airline passengers from Wuhan during February through April.
They then modeled how the disease could spread from those cities if they experienced local outbreaks. Here are 15 of the top 50 destinations that might see outbreaks (also pay attention to the IDVI — the Infectious Disease Vulnerability Index — number. It’s a measure of a country’s ability to manage an infectious disease. Scores closer to zero mean they’re less prepared.)
“By no means would anybody be surprised if there are more cases exported to Europe and the US,” said Bogoch. “But the places that are going to have the greatest volume and number of infections exported would be to East Asian and Southeast Asian centers.”
There are a few ways this outbreak could end, as my colleague Brian Resnickexplained. Perhaps public health measures — identifying cases fast, putting infected people in isolation — will stop the spread of this coronavirus. (That’s what stopped the spread of SARS in 2003.)
Because this is a zoonotic disease, which came from an animal, finding and eliminating that source would also help. Or maybe a vaccine or antiviral will be invented quickly to help curb a broader epidemic (but that’d likely take years).
Finally, there’s the possibility the virus will simply die out. “Disease outbreaks are a bit like fires,” Resnick wrote. “The virus is the flame. Susceptible people are the fuel. Eventually a fire burns itself out if it runs out of kindling. A virus outbreak will end when it stops finding susceptible people to infect.” There’s also the possibility the outbreak doesn’t end, as Nuzzo told Vox, and this simply becomes one of the diseases in circulation that commonly infects humans. How worrying that is again depends on how severe 2019nCoV turns out to be.
A SARS-like virus has sickened thousands in China, and made its way to the United States. Vox’s Julia Belluz explains what’s known and what’s next.
Skinstitut Holiday Gift Kits take the stress out of gifting
Toronto, October 31, 2024 – Beauty gifts are at the top of holiday wish lists this year, and Laser Clinics Canada, a leader in advanced beauty treatments and skincare, is taking the pressure out of seasonal shopping. Today, Laser Clincs Canada announces the arrival of its 2024 Holiday Gift Kits, courtesy of Skinstitut, the exclusive skincare line of Laser Clinics Group.
In time for the busy shopping season, the limited-edition Holiday Gifts Kits are available in Laser Clinics locations in the GTA and Ottawa. Clinics are conveniently located in popular shopping centers, including Hillcrest Mall, Square One, CF Sherway Gardens, Scarborough Town Centre, Rideau Centre, Union Station and CF Markville. These limited-edition Kits are available on a first come, first served basis.
“These kits combine our best-selling products, bundled to address the most relevant skin concerns we’re seeing among our clients,” says Christina Ho, Senior Brand & LAM Manager at Laser Clinics Canada. “With several price points available, the kits offer excellent value and suit a variety of gift-giving needs, from those new to cosmeceuticals to those looking to level up their skincare routine. What’s more, these kits are priced with a savings of up to 33 per cent so gift givers can save during the holiday season.
There are two kits to select from, each designed to address key skin concerns and each with a unique theme — Brightening Basics and Hydration Heroes.
Brightening Basics is a mix of everyday essentials for glowing skin for all skin types. The bundle comes in a sleek pink, reusable case and includes three full-sized products: 200ml gentle cleanser, 50ml Moisture Defence (normal skin) and 30ml1% Hyaluronic Complex Serum. The Brightening Basics kit is available at $129, a saving of 33 per cent.
Hydration Heroes is a mix of hydration essentials and active heroes that cater to a wide variety of clients. A perfect stocking stuffer, this bundle includes four deluxe products: Moisture 15 15 ml Defence for normal skin, 10 ml 1% Hyaluronic Complex Serum, 10 ml Retinol Serum and 50 ml Expert Squalane Cleansing Oil. The kit retails at $59.
In addition to the 2024 Holiday Gifts Kits, gift givers can easily add a Laser Clinic Canada gift card to the mix. Offering flexibility, recipients can choose from a wide range of treatments offered by Laser Clinics Canada, or they can expand their collection of exclusive Skinstitut products.
Brightening Basics 2024 Holiday Gift Kit by Skinstitut, available exclusively at Laser Clincs Canada clinics and online at skinstitut.ca.
Hydration Heroes 2024 Holiday Gift Kit by Skinstitut – available exclusively at Laser Clincs Canada clinics and online at skinstitut.ca.
LONDON (AP) — Most people have accumulated a pile of data — selfies, emails, videos and more — on their social media and digital accounts over their lifetimes. What happens to it when we die?
It’s wise to draft a will spelling out who inherits your physical assets after you’re gone, but don’t forget to take care of your digital estate too. Friends and family might treasure files and posts you’ve left behind, but they could get lost in digital purgatory after you pass away unless you take some simple steps.
Here’s how you can prepare your digital life for your survivors:
Apple
The iPhone maker lets you nominate a “ legacy contact ” who can access your Apple account’s data after you die. The company says it’s a secure way to give trusted people access to photos, files and messages. To set it up you’ll need an Apple device with a fairly recent operating system — iPhones and iPads need iOS or iPadOS 15.2 and MacBooks needs macOS Monterey 12.1.
For iPhones, go to settings, tap Sign-in & Security and then Legacy Contact. You can name one or more people, and they don’t need an Apple ID or device.
You’ll have to share an access key with your contact. It can be a digital version sent electronically, or you can print a copy or save it as a screenshot or PDF.
Take note that there are some types of files you won’t be able to pass on — including digital rights-protected music, movies and passwords stored in Apple’s password manager. Legacy contacts can only access a deceased user’s account for three years before Apple deletes the account.
Google
Google takes a different approach with its Inactive Account Manager, which allows you to share your data with someone if it notices that you’ve stopped using your account.
When setting it up, you need to decide how long Google should wait — from three to 18 months — before considering your account inactive. Once that time is up, Google can notify up to 10 people.
You can write a message informing them you’ve stopped using the account, and, optionally, include a link to download your data. You can choose what types of data they can access — including emails, photos, calendar entries and YouTube videos.
There’s also an option to automatically delete your account after three months of inactivity, so your contacts will have to download any data before that deadline.
Facebook and Instagram
Some social media platforms can preserve accounts for people who have died so that friends and family can honor their memories.
When users of Facebook or Instagram die, parent company Meta says it can memorialize the account if it gets a “valid request” from a friend or family member. Requests can be submitted through an online form.
The social media company strongly recommends Facebook users add a legacy contact to look after their memorial accounts. Legacy contacts can do things like respond to new friend requests and update pinned posts, but they can’t read private messages or remove or alter previous posts. You can only choose one person, who also has to have a Facebook account.
You can also ask Facebook or Instagram to delete a deceased user’s account if you’re a close family member or an executor. You’ll need to send in documents like a death certificate.
TikTok
The video-sharing platform says that if a user has died, people can submit a request to memorialize the account through the settings menu. Go to the Report a Problem section, then Account and profile, then Manage account, where you can report a deceased user.
Once an account has been memorialized, it will be labeled “Remembering.” No one will be able to log into the account, which prevents anyone from editing the profile or using the account to post new content or send messages.
X
It’s not possible to nominate a legacy contact on Elon Musk’s social media site. But family members or an authorized person can submit a request to deactivate a deceased user’s account.
Passwords
Besides the major online services, you’ll probably have dozens if not hundreds of other digital accounts that your survivors might need to access. You could just write all your login credentials down in a notebook and put it somewhere safe. But making a physical copy presents its own vulnerabilities. What if you lose track of it? What if someone finds it?
Instead, consider a password manager that has an emergency access feature. Password managers are digital vaults that you can use to store all your credentials. Some, like Keeper,Bitwarden and NordPass, allow users to nominate one or more trusted contacts who can access their keys in case of an emergency such as a death.
But there are a few catches: Those contacts also need to use the same password manager and you might have to pay for the service.
___
Is there a tech challenge you need help figuring out? Write to us at onetechtip@ap.org with your questions.
The Canadian Paediatric Society says doctors should regularly screen children for reading difficulties and dyslexia, calling low literacy a “serious public health concern” that can increase the risk of other problems including anxiety, low self-esteem and behavioural issues, with lifelong consequences.
New guidance issued Wednesday says family doctors, nurses, pediatricians and other medical professionals who care for school-aged kids are in a unique position to help struggling readers access educational and specialty supports, noting that identifying problems early couldhelp kids sooner — when it’s more effective — as well as reveal other possible learning or developmental issues.
The 10 recommendations include regular screening for kids aged four to seven, especially if they belong to groups at higher risk of low literacy, including newcomers to Canada, racialized Canadians and Indigenous Peoples. The society says this can be done in a two-to-three-minute office-based assessment.
Other tips encourage doctors to look for conditions often seen among poor readers such as attention-deficit hyperactivity disorder; to advocate for early literacy training for pediatric and family medicine residents; to liaise with schools on behalf of families seeking help; and to push provincial and territorial education ministries to integrate evidence-based phonics instruction into curriculums, starting in kindergarten.
Dr. Scott McLeod, one of the authors and chair of the society’s mental health and developmental disabilities committee, said a key goal is to catch kids who may be falling through the cracks and to better connect families to resources, including quicker targeted help from schools.
“Collaboration in this area is so key because we need to move away from the silos of: everything educational must exist within the educational portfolio,” McLeod said in an interview from Calgary, where he is a developmental pediatrician at Alberta Children’s Hospital.
“Reading, yes, it’s education, but it’s also health because we know that literacy impacts health. So I think that a statement like this opens the window to say: Yes, parents can come to their health-care provider to get advice, get recommendations, hopefully start a collaboration with school teachers.”
McLeod noted that pediatricians already look for signs of low literacy in young children by way of a commonly used tool known as the Rourke Baby Record, which offers a checklist of key topics, such as nutrition and developmental benchmarks, to cover in a well-child appointment.
But he said questions about reading could be “a standing item” in checkups and he hoped the society’s statement to medical professionals who care for children “enhances their confidence in being a strong advocate for the child” while spurring partnerships with others involved in a child’s life such as teachers and psychologists.
The guidance said pediatricians also play a key role in detecting and monitoring conditions that often coexist with difficulty reading such as attention-deficit hyperactivity disorder, but McLeod noted that getting such specific diagnoses typically involves a referral to a specialist, during which time a child continues to struggle.
He also acknowledged that some schools can be slow to act without a specific diagnosis from a specialist, and even then a child may end up on a wait list for school interventions.
“Evidence-based reading instruction shouldn’t have to wait for some of that access to specialized assessments to occur,” he said.
“My hope is that (by) having an existing statement or document written by the Canadian Paediatric Society … we’re able to skip a few steps or have some of the early interventions present,” he said.
McLeod added that obtaining specific assessments from medical specialists is “definitely beneficial and advantageous” to know where a child is at, “but having that sort of clear, thorough assessment shouldn’t be a barrier to intervention starting.”
McLeod said the society was partly spurred to act by 2022’s “Right to Read Inquiry Report” from the Ontario Human Rights Commission, which made 157 recommendations to address inequities related to reading instruction in that province.
He called the new guidelines “a big reminder” to pediatric providers, family doctors, school teachers and psychologists of the importance of literacy.
“Early identification of reading difficulty can truly change the trajectory of a child’s life.”
This report by The Canadian Press was first published Oct. 23, 2024.


:no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/19661102/GettyImages_1197720988.jpg)
:no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/19661131/GettyImages_1197630354.jpg)
:no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/19661128/1197627758.jpg.jpg)
:no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/19661119/GettyImages_1197718140.jpg)
:no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/19660954/Screen_Shot_2020_01_31_at_7.00.53_AM.png)