Health Canada’s chief medical adviser says variant-specific vaccines can be approved faster than the general ones first issued to combat COVID-19, but one targeting the Omicron strain still likely won’t be ready in time to help with the latest wave.
Dr. Supriya Sharma said what is really needed are vaccines that can possibly stop more than one variant at a time, including those yet to come.
Omicron became the dominant variant in Canada in just over two weeks, and the Public Health Agency of Canada said Friday it’s now believed to be responsible for more than 90 per cent of all COVID-19 cases.
Studies suggest two doses of the existing mRNA vaccines from Pfizer-BioNTech and Moderna are not good at preventing infection from Omicron.
Multiple studies, however, suggest the vaccines are excellent at keeping symptoms mild, preventing hospitalizations, and shortening the stay and lowering the level of care for those who do get admitted to hospital. Fewer vaccinated Omicron patients, for example, need mechanical ventilation.
Both Pfizer and Moderna are working on new versions of their vaccines that specifically target the Omicron variant.
Moderna is hoping to get its product into trials early this year. Pfizer said it could have 100 million doses of theirs ready as early as March, and Canada has contracts for boosters from both companies that would include vaccines for variants too.
But Sharma said even with the expedited review process for vaccine variants, that’s “probably not” fast enough.
“By that time, based on what we’ve known about the Omicron wave, it might well and truly be through,” she said. “And then the question is always, ‘is there another variant that’s coming up?’”
The solution, she said, likely lies with vaccines that can target more than one variant at a time.
The COVID-19 vaccine technical committee of the World Health Organization said the same thing on Jan. 11, noting Omicron is the fifth variant of concern in two years and “is unlikely to be the last.”
Booster shots that heighten antibody development became the immediate response to Omicron for many governments, including Canada.
Dr. Srinivas Murthy, a British Columbia pediatrician and co-chair of the WHO’s clinical research committee on COVID-19, told The Canadian Press that boosters aren’t a long-term viable option.
“Boosting your way out of a pandemic is going to inevitably shoot you in the foot in the sense that you’re going to have a future variant that’s going to emerge that’s going to cause problems,” he said. “It’s going to evade your vaccines, and then you’re going to have to scramble.”
Omicron doesn’t evade the existing vaccines entirely but a future variant could, he said. The issue largely stems from the fact that the original vaccines train the body’s immune system to recognize what is called the spike protein found on the surface of a virus, and that spike protein is mutating significantly.
Think of the mutated spike protein as a bit of a disguise that makes it harder for the immune system to recognize the virus and mount a defence to kill it off.
Omicron has more than 50 mutations, and at least 36 are on the spike protein.
Multivalent vaccines that use the spike protein from more than one variant, or that target the genetic components of a virus rather than the spike protein, are possibly the ones that could offer protection for both this pandemic and the next novel coronavirus that emerges.
“It’s pan-coronavirus, where it’s looking at big broad neutralizing responses and you don’t have to update it every season and so on,” said Murthy. “That’s been the Holy Grail of flu vaccinology for the past number of decades. We haven’t achieved that yet, because flu is a bit tricky, but we think that it’s achievable for coronavirus, specifically.”
The United States Army has a version heading into Phase 2 trials that can attach multiple spike proteins. A vaccine with the specific spike proteins from all five COVID-19 variants of concern would likely be more successful, even against future variants, because they all share some of the same mutations and what one might miss another may catch.
Moderna is working on trials for multivalent vaccines using combinations of the spike proteins from the original virus and one of the variants, or two of the variants together. It’s not clear when they would be ready for use.
Sharma said even if the vaccines aren’t working as well against variants as they were against the original virus, to her “they’re still miraculous.”
“To have a vaccine that was developed that quickly, that still has, through multiple variants … with boosters, up to 70, 80 per cent effectiveness against serious disease, ailments, hospitalization and death,” she said. “That is miraculous for a new vaccine for a new virus.”
Some Ontario doctors have started offering a free shot that can protect babies from respiratory syncytial virus while Quebec will begin its immunization program next month.
The new shot called Nirsevimab gives babies antibodies that provide passive immunity to RSV, a major cause of serious lower respiratory tract infections for infants and seniors, which can cause bronchiolitis or pneumonia.
Ontario’s ministry of health says the shot is already available at some doctor’s offices in Ontario with the province’s remaining supply set to arrive by the end of the month.
Quebec will begin administering the shots on Nov. 4 to babies born in hospitals and delivery centers.
Parents in Quebec with babies under six months or those who are older but more vulnerable to infection can also book immunization appointments online.
The injection will be available in Nunavut and Yukon this fall and winter, though administration start dates have not yet been announced.
This report by The Canadian Press was first published Oct. 21, 2024.
-With files from Nicole Ireland
Canadian Press health coverage receives support through a partnership with the Canadian Medical Association. CP is solely responsible for this content.
ISLAMABAD (AP) — Polio cases are rising ahead of a new vaccination campaign in Pakistan, where violence targeting health workers and the police protecting them has hampered years of efforts toward making the country polio-free.
Since January, health officials have confirmed 39 new polio cases in Pakistan, compared to only six last year, said Anwarul Haq of the National Emergency Operation Center for Polio Eradication.
The new nationwide drive starts Oct. 28 with the aim to vaccinate at least 32 million children. “The whole purpose of these campaigns is to achieve the target of making Pakistan a polio-free state,” he said.
Pakistan regularly launches campaigns against polio despite attacks on the workers and police assigned to the inoculation drives. Militants falsely claim the vaccination campaigns are a Western conspiracy to sterilize children.
Most of the new polio cases were reported in the southwestern Balochistan and southern Sindh province, following by Khyber Pakhtunkhwa province and eastern Punjab province.
The locations are worrying authorities since previous cases were from the restive northwest bordering Afghanistan, where the Taliban government in September suddenly stopped a door-to-door vaccination campaign.
Afghanistan and Pakistan are the two countries in which the spread of the potentially fatal, paralyzing disease has never been stopped. Authorities in Pakistan have said that the Taliban’s decision will have major repercussions beyond the Afghan border, as people from both sides frequently travel to each other’s country.
The World Health Organization has confirmed 18 polio cases in Afghanistan this year, all but two in the south of the country. That’s up from six cases in 2023. Afghanistan used a house-to-house vaccination strategy this June for the first time in five years, a tactic that helped to reach the majority of children targeted, according to WHO.
Health officials in Pakistan say they want the both sides to conduct anti-polio drives simultaneously.
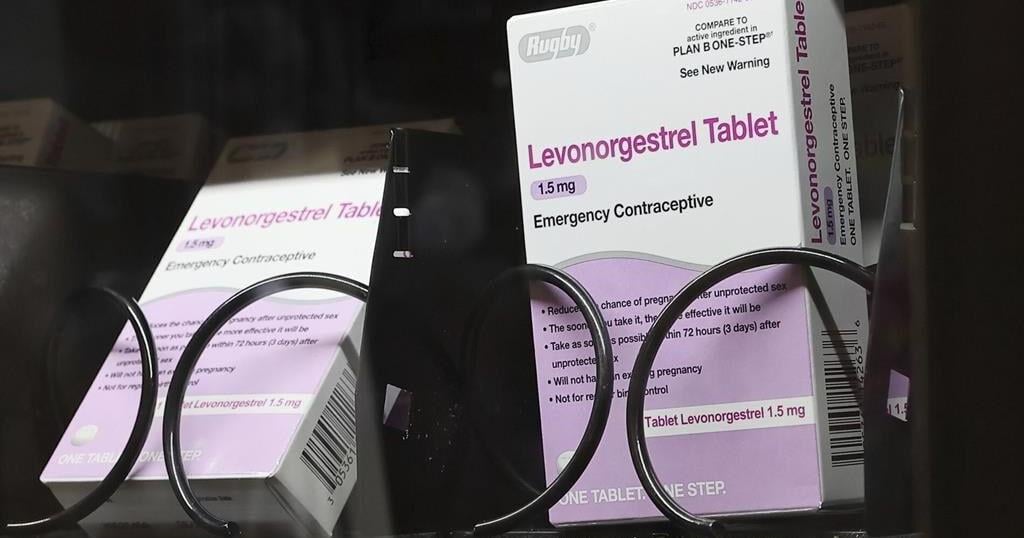
WASHINGTON (AP) — Millions of people with private health insurance would be able to pick up over-the-counter methods like condoms, the “morning after” pill and birth control pills for free under a new rule the White House proposed on Monday.
Right now, health insurers must cover the cost of prescribed contraception, including prescription birth control or even condoms that doctors have issued a prescription for. But the new rule would expand that coverage, allowing millions of people on private health insurance to pick up free condoms, birth control pills, or “morning after” pills from local storefronts without a prescription.
The proposal comes days before Election Day, as Vice President Kamala Harris affixes her presidential campaign to a promise of expanding women’s health care access in the wake of the U.S. Supreme Court’s decision to undo nationwide abortion rights two years ago. Harris has sought to craft a distinct contrast from her Republican challenger, Donald Trump, who appointed some of the judges who issued that ruling.
“The proposed rule we announce today would expand access to birth control at no additional cost for millions of consumers,” Health and Human Services Secretary Xavier Becerra said in a statement. “Bottom line: women should have control over their personal health care decisions. And issuers and providers have an obligation to comply with the law.”
The emergency contraceptives that people on private insurance would be able to access without costs include levonorgestrel, a pill that needs to be taken immediately after sex to prevent pregnancy and is more commonly known by the brand name “Plan B.”
Without a doctor’s prescription, women may pay as much as $50 for a pack of the pills. And women who delay buying the medication in order to get a doctor’s prescription could jeopardize the pill’s effectiveness, since it is most likely to prevent a pregnancy within 72 hours after sex.
If implemented, the new rule would also require insurers to fully bear the cost of the once-a-day Opill, a new over-the-counter birth control pill that the U.S. Food and Drug Administration approved last year. A one-month supply of the pills costs $20.
Federal mandates for private health insurance to cover contraceptive care were first introduced with the Affordable Care Act, which required plans to pick up the cost of FDA-approved birth control that had been prescribed by a doctor as a preventative service.
The proposed rule would not impact those on Medicaid, the insurance program for the poorest Americans. States are largely left to design their own rules around Medicaid coverage for contraception, and few cover over-the-counter methods like Plan B or condoms.