Background: Identifying people with Lynch syndrome, a genetic condition predisposing those affected to colorectal, endometrial and other cancers, allows for implementation of risk-reducing strategies for patients and their families. The goal of this study was to describe screening and testing practices for this condition among people with endometrial cancer in Nova Scotia, Canada, and to determine the prevalence of Lynch syndrome in this population.
Methods: All patients diagnosed with endometrial cancer in Nova Scotia between May 1, 2017, and Apr. 30, 2020 were identified through a provincial gynecologic oncology database. Patients from out of province were excluded. We collected age, body mass index, tumour mismatch repair protein immunohistochemistry results, personal and family histories, and germline testing information for all patients.
Results: We identified 465 people diagosed with endometrial cancer during the study period. Most were aged 51 years or older, and had obesity and low-grade early-stage endometrioid tumours. Tumour immunohistochemistry testing was performed in 444 cases (95.5%). Based on local criteria, 189 patients were eligible for genetic counselling, of whom 156 (82.5%) were referred to medical genetics. Of the 98 patients who underwent germline testing, 9 (9.2%) were diagnosed with Lynch syndrome.
Interpretation: The prevalence of Lynch syndrome was at least 1.9% (9/465) in this population. Our results illustrate successful implementation of universal tumour testing; however, there remains a gap in access to genetic counselling.
Endometrial cancer is the third most common malignant disorder in Canadian females.1 Lynch syndrome (formerly known as hereditary nonpolyposis colorectal cancer) is the leading cause of hereditary endometrial cancer.2 This autosomal dominant condition is caused by inactivating mutations in DNA mismatch repair (MMR) genes, including MLH1, MSH2, MSH6 and PMS2. In addition, there are large deletions in EPCAM, which can lead to transcriptional silencing of MSH2.3 Pathogenic MMR germline mutation confers a high risk of development of a somatic “second-hit” mutation, with subsequent genomic instability and development of cancer in affected people.3 Lynch syndrome has historically been characterized by an increased lifetime risk — 10%–75% — of colorectal cancer.3,4 The lifetime risk of endometrial cancer in females with Lynch syndrome has been reported to exceed that of colorectal cancer, ranging from 8.4% to 71%.3,4 Affected people have a risk of ovarian cancer of 6%–14%, compared to 2%–3% in the general population.1,4 Affected people also have an increased risk of gastric (0.7%–13%), small bowel (0.6%–12%), pancreatic (0.4%–6%) and urothelial (1.9%–15%) cancers.3,4
Screening strategies for Lynch syndrome in people with endometrial cancer include clinical history–based criteria (e.g., Amsterdam and Bethesda criteria5–8), tumour microsatellite instability (MSI) testing and tumour immunohistochemical (IHC) testing. The former identifies DNA repair failures by means of DNA sequencing. In tumour IHC testing, specific antibodies are used to detect MMR protein products of MLH1, MSH2, MSH6 and PMS2. Because MMR proteins form heterodimer pairs, a 4-antibody approach targeting all 4 proteins or a 2-antibody approach targeting only heterodimer partners PMS2 (which binds to MLH1) and MSH6 (which binds to MSH2) may be used.9,10 Tumour MSI and IHC testing have comparable performance; however, MSI testing may not detect abnormalities caused by MSH6 mutations, responsible for a substantial subset of endometrial cancers.10,11 Loss of MLH1 expression on IHC testing is often observed in sporadic cases of endometrial cancer owing to methylation of the MLH1 promoter.12,13 Testing for MLH1 hypermethylation can therefore help differentiate between sporadic and germline pathologic variants.12,13 Tumour testing (MSI or IHC) is recommended to screen for Lynch syndrome in all patients with endometrial cancer, as a substantial number of affected patients do not fulfill clinical history–based criteria.4,14
The prevalence of Lynch syndrome in people with endometrial cancer was reported to be 2.3% in a case series of 543 patients in Ohio and 5% in a cohort of 261 patients in Montréal.15–17 Population and screening strategy differences may explain the higher prevalence in the Montréal cohort. Identifying affected people is crucial to cancer management and in providing risk-reducing strategies for them and their affected relatives.
Nova Scotia introduced universal tumour testing in all endometrial cancer cases in April 2017. To our knowledge, the prevalence of Lynch syndrome in the endometrial cancer population in Nova Scotia has never been described. We aimed to describe screening and testing practices for Lynch syndrome in Nova Scotians with endometrial cancer and to determine the prevalence of Lynch syndrome in that population.
Methods
Setting
In Nova Scotia, all endometrial specimens suggestive of or consistent with malignant disease are reviewed by gynecologic pathologists at a single centre in Halifax. Likewise, all gynecologic cancers diagnosed in the province are treated by gynecologic oncologists in that same centre. Since pathologic review and oncologic care occurs in a single centre, standard of care in this province is established and maintained by close collaboration between the 2 groups. An internal decision was made to perform tumour testing in all endometrial cancer cases, regardless of specimen type, starting Apr. 6, 2017. Two- or 4-stain IHC screening is performed at the discretion of the pathologist, as previously described.18 Testing for MLH1 hypermethylation was not available during the study period (May 1, 2017, to Apr. 30, 2020).
Referral to medical genetics is offered to the patient and then sent by the gynecologic oncologist. In the present study, patients were eligible for genetic counselling if they had 1 or more of the following: any loss of MMR protein expression on tumour IHC testing; age 50 years or younger at the time of diagnosis; personal history of other Lynch-associated malignant disorders, including colorectal, ovarian, gastric, pancreatic, small bowel, urothelial and/or biliary tract cancers; and a family history of Lynch-associated malignant disorders, including endometrial, colorectal, ovarian, gastric, pancreatic, small bowel, urothelial and/or biliary tract cancers, in 2 or more first- or second-degree relatives.
Genetic counselling in Nova Scotia is available only through the Maritime Medical Genetics Service (MMGS), in Halifax. The service offers germline testing to all patients with abnormal results of tumour IHC testing and all patients younger than 40 years, regardless of other risk factors. In patients aged 40 years or older, family history usually guides testing. The same criteria are used in patients with colorectal cancer.
Design
This was a population-based descriptive study using data for all people diagnosed with endometrial cancer in Nova Scotia between May 1, 2017, and Apr. 30, 2020. Patients with a health card number from outside of Nova Scotia were excluded.
Data sources
We used the Tupper Gynaecologic Oncology Database (TGOD) to generate a list of all patients diagnosed with endometrial cancer during the study period. The database contains province-wide data for patients with gynecologic cancers. It is audited for accuracy by its users every few years by comparing provincial cancer statistics. We abstracted age and body mass index at the time of diagnosis, histologic findings, International Federation of Gynaecology and Obstetrics (FIGO) grade and FIGO stage from the database. The TGOD does not contain information on personal or family history. Chart review was then performed for each patient to confirm eligibility and collect missing body mass index information by M.L., an obstetrics and gynecology resident.
Tumour IHC testing results for each patient were extracted from pathology reports by R.W., a pathology resident. The pathology results were double-checked for accuracy by M.L. in about one-third of cases.
Germline testing results, and personal and family histories of Lynch-associated malignant disease for all eligible patients were extracted from medical genetics records by endometrial cancer, MMGS genetic counsellor. All cases identified with a germline mutation or variant of unknown significance, and cases in which patients did not undergo germline testing after referral were verified by M.L. Variants of unknown significance are genetic variants for which there is not enough data to indicate that it clearly increases one’s risk of malignancy or enough data to safely indicate that it does not.
Statistical analysis
We reported age and body mass index using mean and standard deviation. Total numbers and percentages were reported for all other variables. Owing to inadequate statistical power, p values were omitted when comparing groups.
Ethics approval
Ethics approval was obtained from the Nova Scotia Health Research Ethics Board (1026033).
Results
We identified 475 people diagnosed with endometrial cancer between May 1, 2017, and Apr. 30, 2020. Ten patients were excluded, yielding a final cohort of 465 people (Figure 1). Most patients were more than 50 years of age (422 [90.8%]) and had obesity (302/456 [66.2%]), endometrioid histologic subtype (398 [85.6%]), FIGO grade 1 (304/464 [65.4%]) and FIGO stage 1 (338/437 [77.3%]) (Table 1). Personal and family history were unknown in 314 and 320 cases, respectively.
<a href=”https://www.cmajopen.ca/content/cmajo/11/5/E1012/F1.large.jpg?width=800&height=600&carousel=1″ title=”Tumour mismatch repair (MMR) protein testing to screen for Lynch syndrome and referral for genetic counselling in 465 Nova Scotians diagnosed with endometrial cancer between May 1, 2017, and Apr. 30, 2020. *Identified through the Tupper Gynaecologic Oncology Database. †Staining equivocal or suboptimal in 5 cases. ‡Endometrial, colorectal, ovarian, gastric, pancreatic, small bowel, urothelial and/or biliary tract cancers in 2 or more first- or second-degree relatives. §Previous diagnosis of colorectal, ovarian, gastric, pancreatic, small bowel, urothelial and/or biliary tract cancers. ¶At least 1 of the following: loss of expression of 1 or more MMR proteins, age 60 years or less at time of diagnosis, personal history of Lynch-associated malignant disorder or family history of Lynch-associated malignant disorders.” class=”highwire-fragment fragment-images colorbox-load” rel=”gallery-fragment-images-1041752050″ data-figure-caption=”
Tumour mismatch repair (MMR) protein testing to screen for Lynch syndrome and referral for genetic counselling in 465 Nova Scotians diagnosed with endometrial cancer between May 1, 2017, and Apr. 30, 2020. *Identified through the Tupper Gynaecologic Oncology Database. †Staining equivocal or suboptimal in 5 cases. ‡Endometrial, colorectal, ovarian, gastric, pancreatic, small bowel, urothelial and/or biliary tract cancers in 2 or more first- or second-degree relatives. §Previous diagnosis of colorectal, ovarian, gastric, pancreatic, small bowel, urothelial and/or biliary tract cancers. ¶At least 1 of the following: loss of expression of 1 or more MMR proteins, age 60 years or less at time of diagnosis, personal history of Lynch-associated malignant disorder or family history of Lynch-associated malignant disorders.
” data-icon-position data-hide-link-title=”0″>
Figure 1:
Tumour mismatch repair (MMR) protein testing to screen for Lynch syndrome and referral for genetic counselling in 465 Nova Scotians diagnosed with endometrial cancer between May 1, 2017, and Apr. 30, 2020. *Identified through the Tupper Gynaecologic Oncology Database. †Staining equivocal or suboptimal in 5 cases. ‡Endometrial, colorectal, ovarian, gastric, pancreatic, small bowel, urothelial and/or biliary tract cancers in 2 or more first- or second-degree relatives. §Previous diagnosis of colorectal, ovarian, gastric, pancreatic, small bowel, urothelial and/or biliary tract cancers. ¶At least 1 of the following: loss of expression of 1 or more MMR proteins, age 60 years or less at time of diagnosis, personal history of Lynch-associated malignant disorder or family history of Lynch-associated malignant disorders.
View this table:
Table 1:
Participant characteristics
Tumour IHC staining was performed in 444 patients (95.5%), with a 2-stain and a 4-stain panel in 267 and 177 patients, respectively. There was loss of expression of at least 1 protein in 120 patients (27.0%). Different patterns of loss were observed: MLH1 and PMS2 (99 [82.4%]), MSH2 and MSH6 (< 5%), PMS2 only (< 5%), MSH6 only (< 5%), MSH2 only (< 5%), and MLH1, PMS2 and MSH6 (< 1%). Staining gave equivocal or suboptimal results for MLH1 and/or PMS2 in 5 cases; all 5 patients were referred to MMGS.
Of the 465 people, 189 (40.6%) were eligible for genetic counselling; according to medical genetics records, referral was not received for 33 of the 189. Germline testing was offered to 119 (76.3%) of the 156 patients referred, of whom 98 accepted (Figure 2). Germline testing was not offered to 29 of the 156 referred patients (Figure 2). Patients who agreed to undergo germline testing appeared to be more likely than those who declined germline testing to have a personal or family history of Lynch-associated malignant disease; however, the difference was not statistically significant (Table 2). Nine patients were confirmed to have Lynch syndrome, corresponding to 9.2% of those tested and 1.9% of the study population. Seven patients had a variant of unknown significance. Characteristics of the patients with Lynch syndrome are presented in Table 3.
<a href=”https://www.cmajopen.ca/content/cmajo/11/5/E1012/F2.large.jpg?width=800&height=600&carousel=1″ title=”Germline testing in 269 Nova Scotians with endometrial cancer eligible for medical genetics referral. *Testing of peripheral blood to look for pathologic variants associated with Lynch syndrome. †Pathologic variant for Lynch syndrome identified.” class=”highwire-fragment fragment-images colorbox-load” rel=”gallery-fragment-images-1041752050″ data-figure-caption=”
Germline testing in 269 Nova Scotians with endometrial cancer eligible for medical genetics referral. *Testing of peripheral blood to look for pathologic variants associated with Lynch syndrome. †Pathologic variant for Lynch syndrome identified.
” data-icon-position data-hide-link-title=”0″>
Figure 2:
Germline testing in 269 Nova Scotians with endometrial cancer eligible for medical genetics referral. *Testing of peripheral blood to look for pathologic variants associated with Lynch syndrome. †Pathologic variant for Lynch syndrome identified.
View this table:
Table 2:
Characteristics of participants according to whether they accepted or declined germline testing for Lynch syndrome
View this table:
Table 3:
Characteristics of Lynch syndrome cases diagnosed in Nova Scotians with endometrial cancer*
More than half (18 [54%]) of the 33 patients who were not referred to MMGS met the age criteria for referral. Compared to the people who were not referred, those referred appeared to be older, have higher-grade tumours and be more likely to have abnormal results of tumour IHC testing (Table 4).
View this table:
Table 4:
Characteristics of the 189 participants who were eligible for referral to medical genetics according to whether they were referred or not referred
Interpretation
In this study of Nova Scotians diagnosed with endometrial cancer between 2017 and 2020, the prevalence of Lynch syndrome was at least 1.9% (9/465). The patients’ demographic characteristics were similar to those of other populations of patients with endometrial cancer.10–12,15,17,19,20
Personal and family histories were readily available through the genetics database for patients seen by MMGS. These data are not collected in TGOD, and this reflects a gap in data currently being gathered. Although not captured in our database, personal and family histories are typically collected during initial gynecologic oncologic consultations. This information could have been included in our chart review.
Tumour IHC testing was performed in 95.5% of our study population. The reasons why tumour testing was not performed in a minority of patients remain unclear. Overall, uptake of universal tumour testing has been successful since its implementation at our centre, in 2017.
It remains unclear as to why 33 eligible participants were not referred to MMGS. Eighteen of the 33 were eligible for genetic counselling based on age alone. It is possible that patients who met the age criterion for referral to MMGS and had normal results of IHC testing were less interested in pursuing germline testing after discussion with their gynecologic oncologist. A minority of patients may have already been diagnosed with a family cancer syndrome, remotely or in another province. This could not be captured in our data. Notably, 16 patients not referred to MMGS had abnormal tumour testing results.
Despite successful implementation of universal tumour testing, access to genetic counselling remains a challenge. We agree with Dicks and colleagues19 that the success of programs offering universal tumour screening for Lynch syndrome ultimately depends on patients’ being able to access germline testing after receiving a positive screening result. Barriers to accessing genetic counselling identified in their survey of Canadian pathologists and genetic counsellors included lack of counsellors and lack of an interdisciplinary approach.19 Our centre uses an inclusive interdisciplinary approach, with weekly case rounds attended by pathologists, radiologists, gynecologic oncologists and genetic counsellors; however, not all patients are discussed during these rounds. Other possible barriers include patients’ being too unwell and/or declining referral when offered by their gynecologic oncologist. This could not be captured in our data.
Germline testing confirmed 9 cases of Lynch syndrome and showed 7 variants of unknown significance. Such patients should be seen by medical genetics every few years for updated information on their variant. Among the confirmed cases of Lynch syndrome, PMS2 mutations were found in the 3 oldest patients. This is consistent with literature reports of PMS2’s having the lowest penetrance and generally manifesting later in life compared to other variants.3 One patient had normal results of tumour IHC testing. Although such testing is the most effective screening strategy for Lynch syndrome, 11,12,14,20 family history remains clinically relevant. A small number of patients may be missed when IHC testing alone is relied on,11,12,15 as staining may be intact for some nonfunctioning mutant proteins.10 The sensitivity and specificity of IHC testing in identifying patients with Lynch syndrome at our institution is unknown; however, participation in an external quality-assurance program conducted by Canadian Pathology Quality Assurance showed 98.1% accuracy for our MMR IHC stains in 2021–2022.
The prevalence of Lynch syndrome in our population is similar to that in a previously described US population15,16 but, interestingly, is less than half that reported in a cohort of Montréal patients.17 At the time of writing, germline status remained unknown for 91 of the 189 participants eligible for genetic counselling. Our criteria for referral to medical genetics were broader than those in the studies by Hampel and colleagues15 and Lawrence and colleagues.17 In both studies, only tumour testing, including MLH1-hypermethylation testing, was used to triage patients. If we had done the same, only 15 patients would not have been referred (compared to 33). The uptake of germline testing in our population was also lower than that in those studies,15,17 with 21 patients declining testing and 11 patients declining consultation with MMGS. It is difficult to make conclusions regarding the true prevalence of Lynch syndrome in our population; however, given the sensitivity of IHC testing and the uptake of germline testing in our study, our estimate is likely an underestimate.
This project allowed us to identify specific knowledge and service gaps. Our clinical pathways are being reviewed to ensure that testing is available to all appropriate patients. The TGOD continues to undergo quality review, and further validation, including improvement in the type of data collected and data accuracy, is planned. As the responsibility to refer to MMGS typically falls on the gynecologic oncologists, adding a variable regarding genetic testing in TGOD may be useful. Ideally, results of tumour IHC testing should be available at initial consultation, and MMGS referral considered and sent then. Educating patients to improve their knowledge of the benefits of genetic testing is currently a priority.
Sending pathology reports of abnormal IHC testing results directly to genetic counsellors could also be considered to ensure better referral rates. The age criterion for referral could be reviewed, as some patients meeting the current criterion may not qualify for germline testing. Testing for MLH1 hypermethylation should also help reduce referral volumes. We hope that modifying clinical pathways to lower referral volumes will decrease wait times, which, in turn, may lessen barriers to accessing germline testing such as inability to be contacted owing to change in contact information and death from disease while awaiting an appointment. Other strategies to decrease wait times may include hiring more genetic counsellors and offering group counselling for specific indications.19
Limitations
The use of province-wide data and a relatively large population were strengths of this study. A major limitation was the inability to determine why patients were not referred to MMGS. Other limitations include retrospective data collection through databases, and the lack of data on body mass index and personal and family histories. As our population was geographically restricted to Nova Scotia, our results may not be generalizable to other populations. Owing to the small number of patients with Lynch syndrome, the accuracy of our tumour IHC testing and our ability to compare germline mutations to those of other populations are limited; this may be feasible as part of a larger project in the future.
Conclusion
The prevalence of Lynch syndrome in our study population of patients with endometrial cancer, 1.9%, was similar to that reported for other populations. Our results show successful implementation of universal tumour testing; however, there remains a gap in access to genetic counselling. Clinical pathways ensuring access to genetic counselling for all eligible people are necessary for prompt diagnosis of Lynch syndrome in patients and their family members in order to implement risk-reducing strategies.
Acknowledgement
The authors acknowledge Erin Chamberlain, a Canadian certified genetic counsellor with the Maritime Medical Genetics Service, for providing medical genetics data and insight from a medical genetics’ perspective.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Marianne Levesque and Katharina Kieser conceived and designed the project. Katharina Kieser supervised the project. Richard Wood collected the pathology data. Marianne Levesque collected the demographic and oncologic data, and oversaw data merging and coding. Marianne Levesque supervised data analysis, which was provided in part by a third party (Nova Scotia Health’s Research Methods Unit), and drafted the manuscript. Marianne Levesque, Katharina Kieser and Michael Carter intrepreted the data. Richard Wood, Michael Carter, Jo-Ann Brock and Katharina Kieser revised the manuscript critically for important intellectual content. All authors approved the final version to be published and agreed to be accountable for all aspects of the work.
Funding: Funding for this study was obtained from the Department of Obstetrics and Gynaecology, Dalhousie University, Halifax, Nova Scotia.
Data sharing: Given the small size of and identifiable content in the Tupper Gynaecologic Oncology Database, data from the database are available only to those directly involved in patient care in our institution. Data used in this study are available in an unidentified, coded format from the first author on reasonable request: Marianne.levesqueatdal.ca.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
Some Ontario doctors have started offering a free shot that can protect babies from respiratory syncytial virus while Quebec will begin its immunization program next month.
The new shot called Nirsevimab gives babies antibodies that provide passive immunity to RSV, a major cause of serious lower respiratory tract infections for infants and seniors, which can cause bronchiolitis or pneumonia.
Ontario’s ministry of health says the shot is already available at some doctor’s offices in Ontario with the province’s remaining supply set to arrive by the end of the month.
Quebec will begin administering the shots on Nov. 4 to babies born in hospitals and delivery centers.
Parents in Quebec with babies under six months or those who are older but more vulnerable to infection can also book immunization appointments online.
The injection will be available in Nunavut and Yukon this fall and winter, though administration start dates have not yet been announced.
This report by The Canadian Press was first published Oct. 21, 2024.
-With files from Nicole Ireland
Canadian Press health coverage receives support through a partnership with the Canadian Medical Association. CP is solely responsible for this content.
ISLAMABAD (AP) — Polio cases are rising ahead of a new vaccination campaign in Pakistan, where violence targeting health workers and the police protecting them has hampered years of efforts toward making the country polio-free.
Since January, health officials have confirmed 39 new polio cases in Pakistan, compared to only six last year, said Anwarul Haq of the National Emergency Operation Center for Polio Eradication.
The new nationwide drive starts Oct. 28 with the aim to vaccinate at least 32 million children. “The whole purpose of these campaigns is to achieve the target of making Pakistan a polio-free state,” he said.
Pakistan regularly launches campaigns against polio despite attacks on the workers and police assigned to the inoculation drives. Militants falsely claim the vaccination campaigns are a Western conspiracy to sterilize children.
Most of the new polio cases were reported in the southwestern Balochistan and southern Sindh province, following by Khyber Pakhtunkhwa province and eastern Punjab province.
The locations are worrying authorities since previous cases were from the restive northwest bordering Afghanistan, where the Taliban government in September suddenly stopped a door-to-door vaccination campaign.
Afghanistan and Pakistan are the two countries in which the spread of the potentially fatal, paralyzing disease has never been stopped. Authorities in Pakistan have said that the Taliban’s decision will have major repercussions beyond the Afghan border, as people from both sides frequently travel to each other’s country.
The World Health Organization has confirmed 18 polio cases in Afghanistan this year, all but two in the south of the country. That’s up from six cases in 2023. Afghanistan used a house-to-house vaccination strategy this June for the first time in five years, a tactic that helped to reach the majority of children targeted, according to WHO.
Health officials in Pakistan say they want the both sides to conduct anti-polio drives simultaneously.
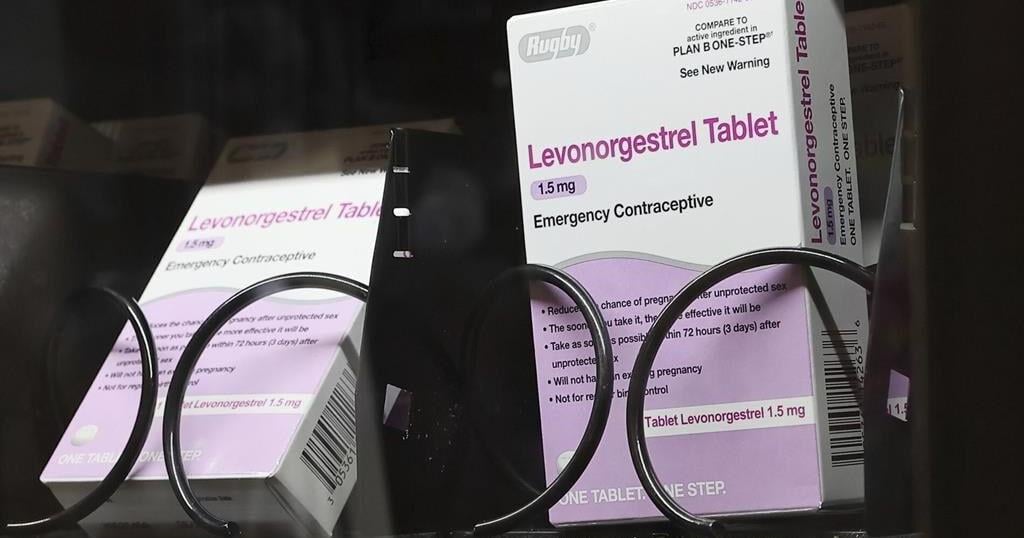
WASHINGTON (AP) — Millions of people with private health insurance would be able to pick up over-the-counter methods like condoms, the “morning after” pill and birth control pills for free under a new rule the White House proposed on Monday.
Right now, health insurers must cover the cost of prescribed contraception, including prescription birth control or even condoms that doctors have issued a prescription for. But the new rule would expand that coverage, allowing millions of people on private health insurance to pick up free condoms, birth control pills, or “morning after” pills from local storefronts without a prescription.
The proposal comes days before Election Day, as Vice President Kamala Harris affixes her presidential campaign to a promise of expanding women’s health care access in the wake of the U.S. Supreme Court’s decision to undo nationwide abortion rights two years ago. Harris has sought to craft a distinct contrast from her Republican challenger, Donald Trump, who appointed some of the judges who issued that ruling.
“The proposed rule we announce today would expand access to birth control at no additional cost for millions of consumers,” Health and Human Services Secretary Xavier Becerra said in a statement. “Bottom line: women should have control over their personal health care decisions. And issuers and providers have an obligation to comply with the law.”
The emergency contraceptives that people on private insurance would be able to access without costs include levonorgestrel, a pill that needs to be taken immediately after sex to prevent pregnancy and is more commonly known by the brand name “Plan B.”
Without a doctor’s prescription, women may pay as much as $50 for a pack of the pills. And women who delay buying the medication in order to get a doctor’s prescription could jeopardize the pill’s effectiveness, since it is most likely to prevent a pregnancy within 72 hours after sex.
If implemented, the new rule would also require insurers to fully bear the cost of the once-a-day Opill, a new over-the-counter birth control pill that the U.S. Food and Drug Administration approved last year. A one-month supply of the pills costs $20.
Federal mandates for private health insurance to cover contraceptive care were first introduced with the Affordable Care Act, which required plans to pick up the cost of FDA-approved birth control that had been prescribed by a doctor as a preventative service.
The proposed rule would not impact those on Medicaid, the insurance program for the poorest Americans. States are largely left to design their own rules around Medicaid coverage for contraception, and few cover over-the-counter methods like Plan B or condoms.