You may have heard of Ozempic, the “miracle drug” for weight loss, but did you know that it was actually designed as a new treatment to manage diabetes? In Canada, diabetes affects approximately 10 per cent of the general population. Of those cases, 90 per cent have Type 2 diabetes.
This metabolic disorder is characterized by persistent high blood sugar levels, which can be accompanied by secondary health challenges, including a higher risk of stroke and kidney disease.
Locks and keys
In Type 2 diabetes, the body struggles to maintain blood sugar levels in an acceptable range. Every cell in the body needs sugar as an energy source, but too much sugar can be toxic to cells. This equilibrium needs to be tightly controlled and is regulated by a lock and key system.
In the body’s attempt to manage blood sugar levels and ensure that cells receive the right amount of energy, the pancreatic hormone, insulin, functions like a key. Cells cover themselves with locks that respond perfectly to insulin keys to facilitate the entry of sugar into cells.
Unfortunately, this lock and key system doesn’t always perform as expected. The body can encounter difficulties producing an adequate number of insulin keys, and/or the locks can become stubborn and unresponsive to insulin.
All forms of diabetes share the challenge of high blood sugar levels; however, diabetes is not a singular condition; it exists as a spectrum. Although diabetes is broadly categorized into two main types, Type 1 and Type 2, each presents a diversity of subtypes, especially Type 2 diabetes.
To better serve people living with Type 2 diabetes, and to move away from a “one size fits all” approach, it is beneficial to understand which subtype of Type 2 diabetes a person lives with. When someone needs a blood transfusion, the medical team needs to know the patient’s blood type. It should be the same for diabetes so a tailored and effective game plan can be implemented.
This article explores four unique subtypes of Type 2 diabetes, shedding light on their causes, complications and some of their specific treatment avenues.
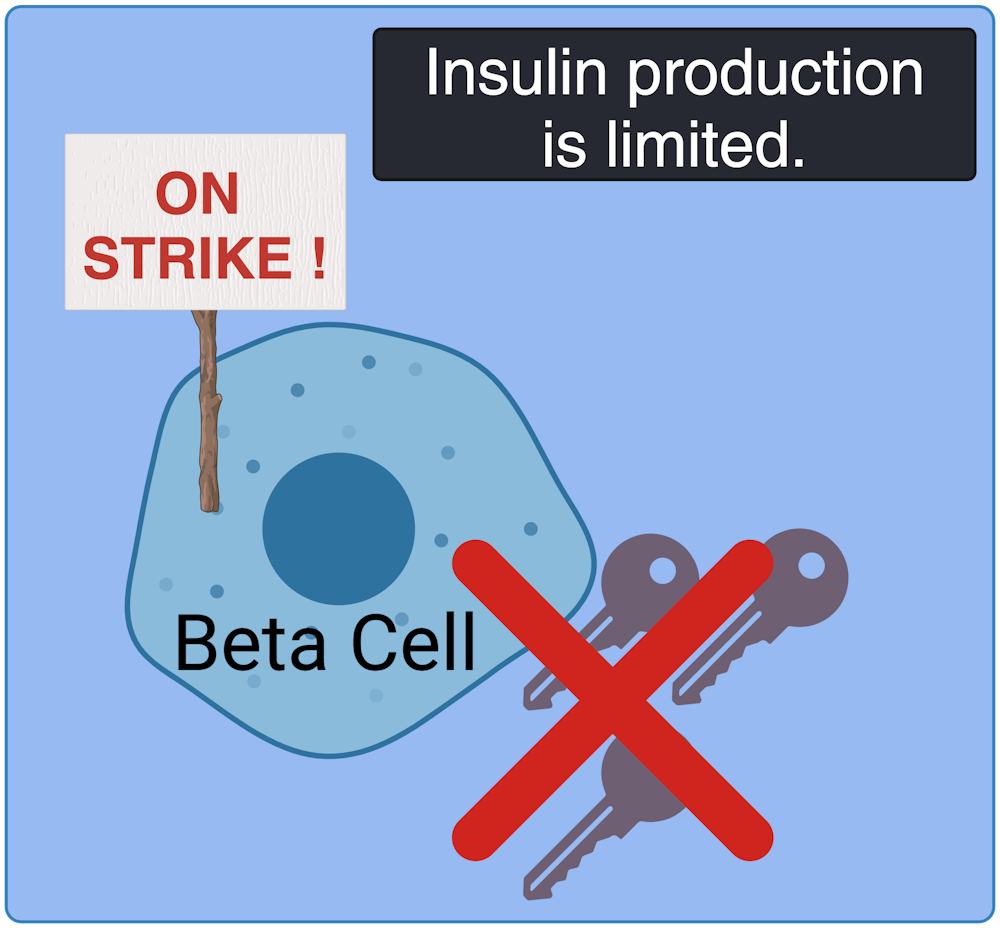
Severe insulin-deficient diabetes: We’re missing keys!
In severe insulin-deficient diabetes, beta cells limit production of the keys that unlock cells to allow entry of sugar from the blood. (Lili Grieco-St-Pierre, Jennifer Bruin/Created with BioRender.com)
Insulin is produced by beta cells, which are found in the pancreas. In the severe insulin-deficient diabetes (SIDD) subtype, the key factories — the beta cells — are on strike. Ultimately, there are fewer keys in the body to unlock the cells and allow entry of sugar from the blood.
SIDD primarily affects younger, leaner individuals, and unfortunately, increases the risk of eye disease and blindness, among other complications. Why the beta cells go on strike remains largely unknown, but since there is an insulin deficiency, treatment often involves insulin injections.
Severe insulin-resistant diabetes: But it’s always locked!
In severe insulin-resistant diabetes, the locks start ignoring the keys, triggering the beta cells to produce even more keys to compensate. (Lili Grieco-St-Pierre, Jennifer Bruin/Created with BioRender.com)
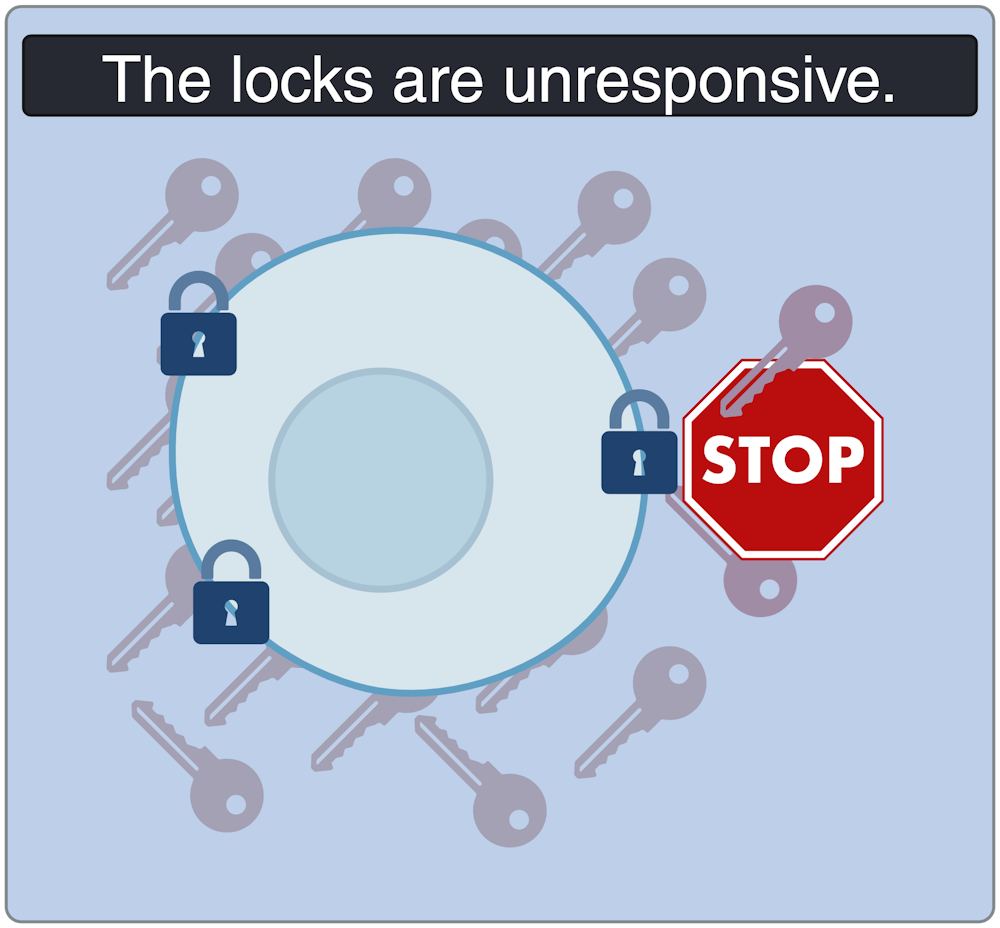
In the severe insulin-resistant diabetes (SIRD) subtype, the locks are overstimulated and start ignoring the keys. As a result, the beta cells produce even more keys to compensate. This can be measured as high levels of insulin in the blood, also known as hyperinsulinemia.
Mild obesity-related diabetes: The locks are sticky!
In mild obesity-related diabetes, the locks are ‘sticky,’ making it difficult for the keys to open the locks. (Lili Grieco-St-Pierre, Jennifer Bruin/Created with BioRender.com)
Mild obesity-related (MOD) diabetes represents a nuanced aspect of Type 2 diabetes, often observed in individuals with higher body weight. Unlike more severe subtypes, MOD is characterized by a more measured response to insulin. The locks are “sticky,” so it is challenging for the key to click in place and open the lock. While MOD is connected to body weight, the comparatively less severe nature of MOD distinguishes it from other diabetes subtypes.
To minimize complications, treatment should include maintaining a healthy diet, managing body weight, and incorporating as much aerobic exercise as possible. This is where drugs like Ozempic can be prescribed to control the evolution of the disease, in part by managing body weight.
Mild age-related diabetes: I’m tired of controlling blood sugar!
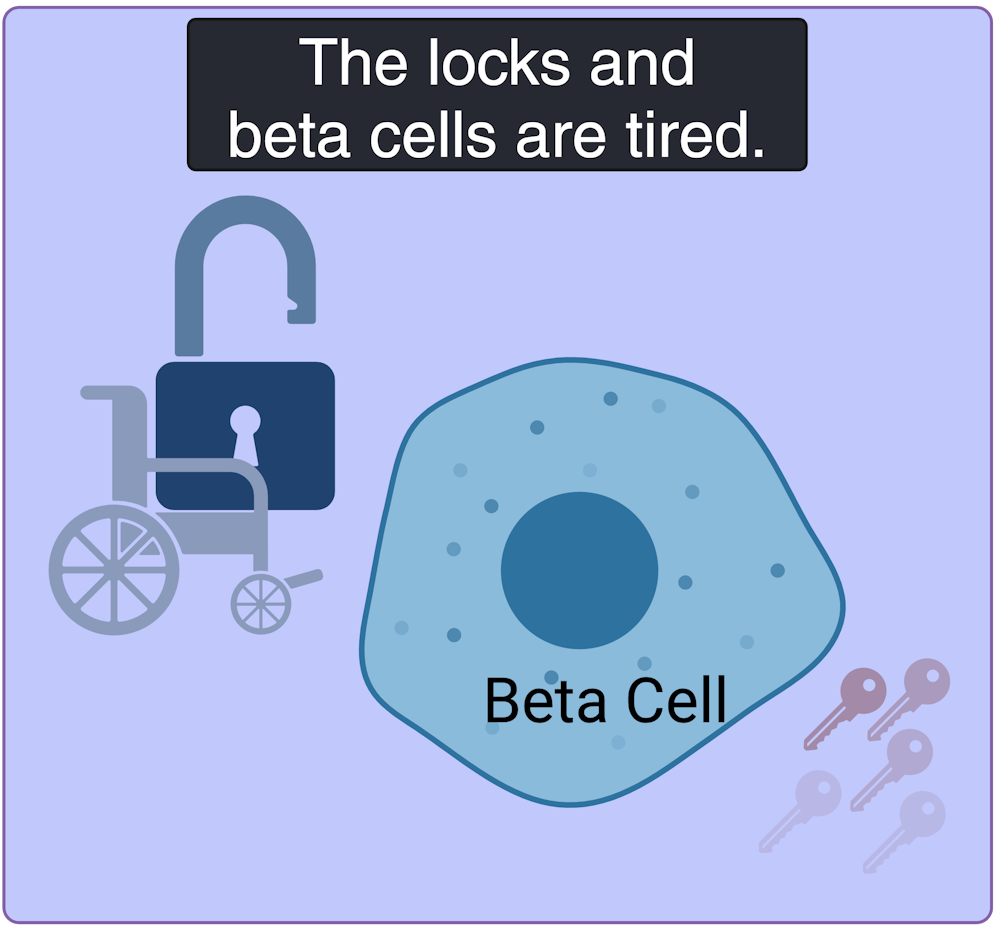
In people with mild age-related diabetes, both the locks and the beta cells that produce keys are tired, resulting in fewer keys and stubborn locks. (Lili Grieco-St-Pierre, Jennifer Bruin/Created with BioRender.com)
Mild age-related diabetes (MARD) happens more often in older people and typically starts later in life. With time, the key factory is not as productive, and the locks become stubborn. People with MARD find it tricky to manage their blood sugar, but it usually doesn’t lead to severe complications.
While efforts have been made to classify diabetes subtypes, new subtypes are still being identified, making proper clinical assessment and treatment plans challenging.
In Canada, unique cases of Type 2 diabetes were identified in Indigenous children from Northern Manitoba and Northwestern Ontario by Dr. Heather Dean and colleagues in the 1980s and 90s. Despite initial skepticism from the scientific community, which typically associated Type 2 diabetes with adults rather than children, clinical teams persisted in identifying this as a distinct subtype of Type 2 diabetes, called childhood-onset Type 2 diabetes.
Acknowledging this distinct subtype of Type 2 diabetes in First Nations communities has led to the implementation of a community-based health action plan aimed at addressing the unique challenges faced by Indigenous Peoples. It is hoped that partnered research between communities and researchers will continue to help us understand childhood-onset Type 2 diabetes and how to effectively prevent and treat it.
A mosaic of conditions
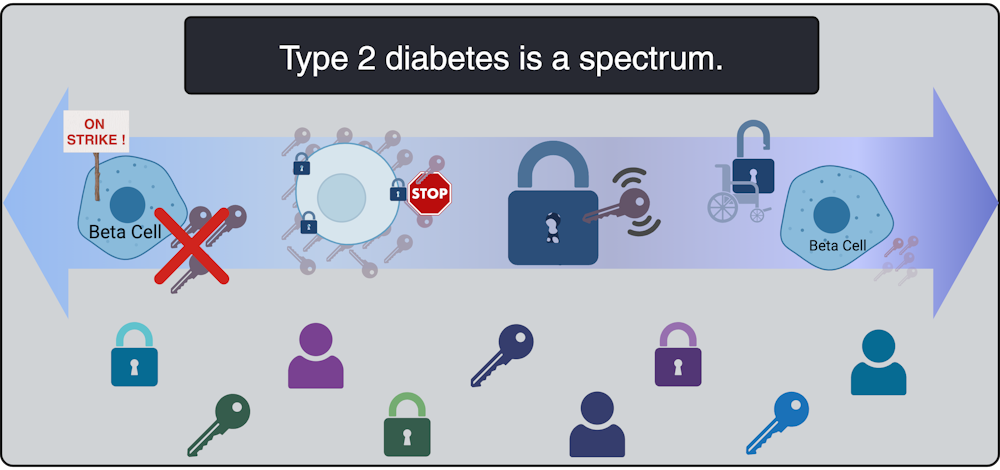
Type 2 diabetes is a mosaic of conditions, each with its own characteristics. (Lili Grieco-St-Pierre, Jennifer Bruin/Created with BioRender.com)
Type 2 diabetes is not uniform; it’s a mosaic of conditions, each with its own characteristics. Since diabetes presents so uniquely in every patient, even categorizing into subtypes does not guarantee how the disease will evolve. However, understanding these subtypes is a good starting point to help doctors create personalized plans for people living with the condition.
While Indigenous communities, lower-income households and individuals living with obesity already face a higher risk of developing Type 2 diabetes than the general population, tailored solutions may offer hope for better management. This emphasizes the urgent need for more precise assessments of diabetes subtypes to help customize therapeutic strategies and management strategies. This will improve care for all patients, including those from vulnerable and understudied populations.
Some Ontario doctors have started offering a free shot that can protect babies from respiratory syncytial virus while Quebec will begin its immunization program next month.
The new shot called Nirsevimab gives babies antibodies that provide passive immunity to RSV, a major cause of serious lower respiratory tract infections for infants and seniors, which can cause bronchiolitis or pneumonia.
Ontario’s ministry of health says the shot is already available at some doctor’s offices in Ontario with the province’s remaining supply set to arrive by the end of the month.
Quebec will begin administering the shots on Nov. 4 to babies born in hospitals and delivery centers.
Parents in Quebec with babies under six months or those who are older but more vulnerable to infection can also book immunization appointments online.
The injection will be available in Nunavut and Yukon this fall and winter, though administration start dates have not yet been announced.
This report by The Canadian Press was first published Oct. 21, 2024.
-With files from Nicole Ireland
Canadian Press health coverage receives support through a partnership with the Canadian Medical Association. CP is solely responsible for this content.
ISLAMABAD (AP) — Polio cases are rising ahead of a new vaccination campaign in Pakistan, where violence targeting health workers and the police protecting them has hampered years of efforts toward making the country polio-free.
Since January, health officials have confirmed 39 new polio cases in Pakistan, compared to only six last year, said Anwarul Haq of the National Emergency Operation Center for Polio Eradication.
The new nationwide drive starts Oct. 28 with the aim to vaccinate at least 32 million children. “The whole purpose of these campaigns is to achieve the target of making Pakistan a polio-free state,” he said.
Pakistan regularly launches campaigns against polio despite attacks on the workers and police assigned to the inoculation drives. Militants falsely claim the vaccination campaigns are a Western conspiracy to sterilize children.
Most of the new polio cases were reported in the southwestern Balochistan and southern Sindh province, following by Khyber Pakhtunkhwa province and eastern Punjab province.
The locations are worrying authorities since previous cases were from the restive northwest bordering Afghanistan, where the Taliban government in September suddenly stopped a door-to-door vaccination campaign.
Afghanistan and Pakistan are the two countries in which the spread of the potentially fatal, paralyzing disease has never been stopped. Authorities in Pakistan have said that the Taliban’s decision will have major repercussions beyond the Afghan border, as people from both sides frequently travel to each other’s country.
The World Health Organization has confirmed 18 polio cases in Afghanistan this year, all but two in the south of the country. That’s up from six cases in 2023. Afghanistan used a house-to-house vaccination strategy this June for the first time in five years, a tactic that helped to reach the majority of children targeted, according to WHO.
Health officials in Pakistan say they want the both sides to conduct anti-polio drives simultaneously.
WASHINGTON (AP) — Millions of people with private health insurance would be able to pick up over-the-counter methods like condoms, the “morning after” pill and birth control pills for free under a new rule the White House proposed on Monday.
Right now, health insurers must cover the cost of prescribed contraception, including prescription birth control or even condoms that doctors have issued a prescription for. But the new rule would expand that coverage, allowing millions of people on private health insurance to pick up free condoms, birth control pills, or “morning after” pills from local storefronts without a prescription.
The proposal comes days before Election Day, as Vice President Kamala Harris affixes her presidential campaign to a promise of expanding women’s health care access in the wake of the U.S. Supreme Court’s decision to undo nationwide abortion rights two years ago. Harris has sought to craft a distinct contrast from her Republican challenger, Donald Trump, who appointed some of the judges who issued that ruling.
“The proposed rule we announce today would expand access to birth control at no additional cost for millions of consumers,” Health and Human Services Secretary Xavier Becerra said in a statement. “Bottom line: women should have control over their personal health care decisions. And issuers and providers have an obligation to comply with the law.”
The emergency contraceptives that people on private insurance would be able to access without costs include levonorgestrel, a pill that needs to be taken immediately after sex to prevent pregnancy and is more commonly known by the brand name “Plan B.”
Without a doctor’s prescription, women may pay as much as $50 for a pack of the pills. And women who delay buying the medication in order to get a doctor’s prescription could jeopardize the pill’s effectiveness, since it is most likely to prevent a pregnancy within 72 hours after sex.
If implemented, the new rule would also require insurers to fully bear the cost of the once-a-day Opill, a new over-the-counter birth control pill that the U.S. Food and Drug Administration approved last year. A one-month supply of the pills costs $20.
Federal mandates for private health insurance to cover contraceptive care were first introduced with the Affordable Care Act, which required plans to pick up the cost of FDA-approved birth control that had been prescribed by a doctor as a preventative service.
The proposed rule would not impact those on Medicaid, the insurance program for the poorest Americans. States are largely left to design their own rules around Medicaid coverage for contraception, and few cover over-the-counter methods like Plan B or condoms.




























{kind=link}