







 Can I share this graphic?
Can I share this graphic? When do I need a license?
When do I need a license? Interested in this piece?
Interested in this piece?a.bg-showmore-plg-link:hover,a.bg-showmore-plg-link:active,a.bg-showmore-plg-link:focuscolor:#0071bb;
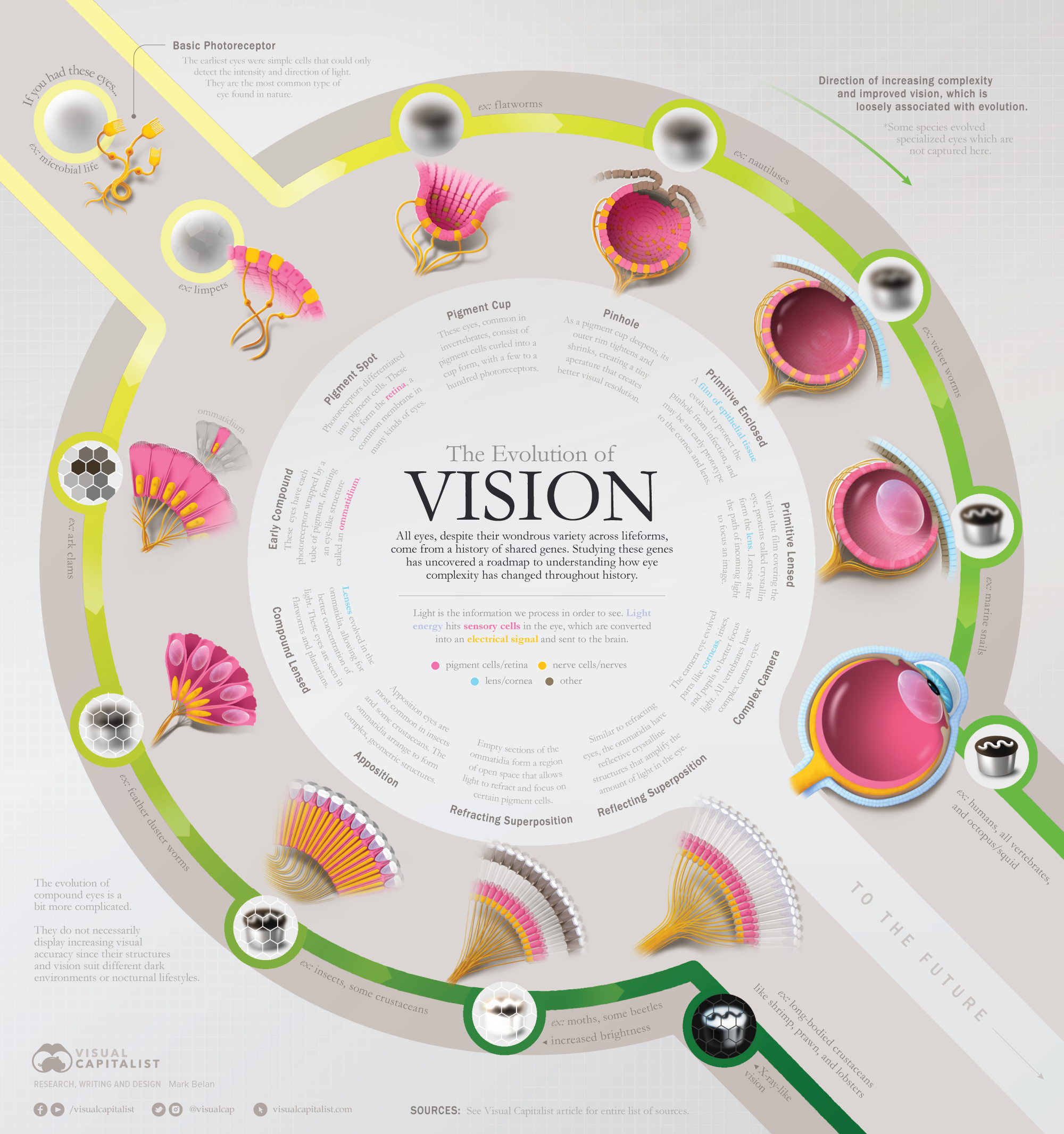
Roadmapping the Evolution of the Eye
Throughout history, numerous creatures have evolved increasingly complex eyes in response to different selective pressures.
Not all organisms, however, experience the same pressures. It’s why some creatures today still have eyes that are quite simple, or why some have no eyes at all. These organisms exemplify eyes that are “frozen” in time. They provide snapshots of the past, or “checkpoints” of how the eye has transformed throughout its evolutionary journey.
Scientists study the genes, anatomy, and vision of these creatures to figure out a roadmap of how the eye came to be. And so, we put together an evolutionary graphic timeline of the eye’s different stages using several candidate species.
Let’s take a look at how the eye has formed throughout time.
Where Vision Comes From
The retina is a layer of nerve tissue, often at the back of the eye, that is sensitive to light.
When light hits it, specialized cells called photoreceptors transform light energy into electrical signals and send them to the brain. Then the brain processes these electrical signals into images, creating vision.
The earliest form of vision arose in unicellular organisms. Containing simple nerve cells that can only distinguish light from dark, they are the most common eye in existence today.
The ability to detect shapes, direction, and color comes from all of the add-ons evolution introduces to these cells.
Two Major Types of Eyes
Two major eye types are dominant across species. Despite having different shapes or specialized parts, improved vision in both eye types is a product of small, gradual changes that optimize the physics of light.
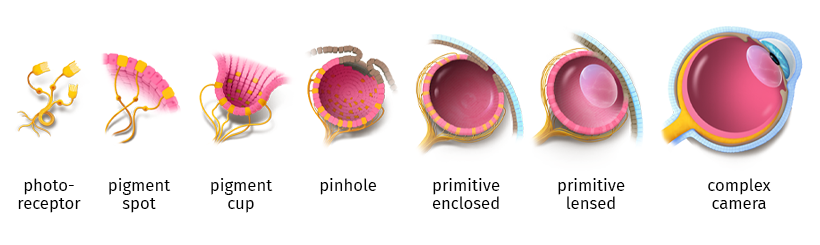
Simple Eyes
Simple eyes are actually quite complex, but get their name because they consist of one individual unit.
Some mollusks and all of the higher vertebrates, like birds, reptiles, or humans, have simple eyes.

Simple eyes evolved from a pigment cup, slowly folding inwards with time into the shape we recognize today. Specialized structures like the lens, cornea, and pupil arose to help improve the focus of light on the retina. This helps create sharper, clearer images for the brain to process.
Compound Eyes
Compound eyes are formed by repeating the same basic units of photoreceptors called ommatidia. Each ommatidium is similar to a simple eye, composed of lenses and photoreceptors.
Grouped together, ommatidia form a geodesic pattern that is commonly seen in insects and crustaceans.

Our understanding of the evolution of the compound eye is a bit murky, but we know that rudimentary ommatidia evolved into larger, grouped structures that maximize light capture.
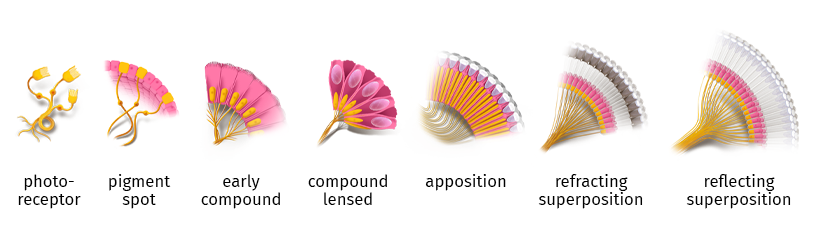
In environments like caves, the deep subsurface, or the ocean floor where little to no light exists, compound eyes are useful for producing vision that gives even the slightest advantage over other species.
How Will Vision Evolve?
Our increasing dependency on technology and digital devices may be ushering in the advent of a new eye shape.
The muscles around the eye stretch to shift the lens when staring at something close by. The eye’s round shape elongates in response to this muscle strain.
Screen time with cellphones, tablets, and computers has risen dramatically over the years, especially during the COVID-19 pandemic. Recent studies are already reporting rises in childhood myopia, the inability to see far away. Since the pandemic, cases have increased by 17%, affecting almost 37% of schoolchildren.
Other evolutionary opportunities for our eyes are currently less obvious. It remains to be seen whether advanced corrective therapies, like corneal transplants or visual prosthetics, will have any long-term evolutionary impact on the eye.
For now, colored contacts and wearable tech may be our peek into the future of vision.
Complete Sources
Fernald, Russell D. “Casting a Genetic Light on the Evolution of Eyes.” Science, vol. 313, no. 5795, 29 Sept. 2006, pp. 1914–1918
Gehring, W. J. “New Perspectives on Eye Development and the Evolution of Eyes and Photoreceptors.” Journal of Heredity, vol. 96, no. 3, 13 Jan. 2005, pp. 171–184. Accessed 18 Dec. 2019.
“The Evolution of Sight | PHOS.”
Land, Michael F, and Dan-Eric Nilsson. Animal Eyes. Oxford ; New York, Oxford University Press, 2002.
“The Major Topics of the Research Work of Prof. Dan-E. Nilsson: Vision-Research.eu – the Gateway to European Vision Research.” Accessed 3 Oct. 2022.








