




")


On Monday, a press release from the transnational pharmaceutical company Pfizer dropped a rare spark of hope into the ongoing misery of the COVID-19 pandemic. Yes, new infections have hit an all-time high in the United States, and, yes, cities and states around the world are walking back their reopenings. But Pfizer says it has results from a massive clinical trial showing that its vaccine against the disease works, and works well. The release touted “a vaccine efficacy rate above 90 percent,” and it announced the company’s intention to seek from the US Food and Drug Administration an authorization to start giving people shots. The company’s ready to make 50 million doses this year and 1.3 billion doses in 2021.
That’s an ember of hope, but it’s sitting under a bucket of cold water, ready to pour. The Pfizer vaccine is finicky—hard to make, transport, and deliver. Because of desperate need, it’s in short supply even before it becomes available—1.3 billion doses is several billion short of what the world needs. The press release wasn’t peer-reviewed science, and it lacked critical details about how the vaccine works and on whom. Even the simple fact of this vaccine’s existence, some analysts have argued, might jeopardize the testing and success of potentially better vaccines down the line, a case of the imperfect being the enemy of the good.
Before the ember dies out completely, here’s a theory: no. The Pfizer vaccine’s imperfections make it a perfect prime mover, because if it works as well as the company says, it’ll help people now and require research into more, better, different vaccines for later. All the things nobody knows about the Pfizer vaccine mean that the door is wide open. “Whether its effects are durable, whether it’s effective in the elderly, whether it has safety issues, the cold chain issues, the ability to have access,” says Wayne Koff, president and CEO of the nonprofit Human Vaccines Project, “all that points to the need for a number of vaccines.”
Working with a smaller company called BioNTech, Pfizer moved off the starting block fast, and without the money from the US Operation Warp Speed program that funded other drug companies’ trials. This vaccine (like another candidate made by the company Moderna) is actually a tailored bit of genetic material called messenger RNA; give it to people, and the mRNA acts like biological software, teaching cells to manufacture the “spike” protein on the outer coat of the virus that causes COVID-19. Those people’s immune systems then learn to recognize and attack the spike, which gives them the ability to fight the virus. It’s a cool idea, and as my colleague Megan Molteni has written, it could change the future of vaccinology and infectious disease.
Cold case
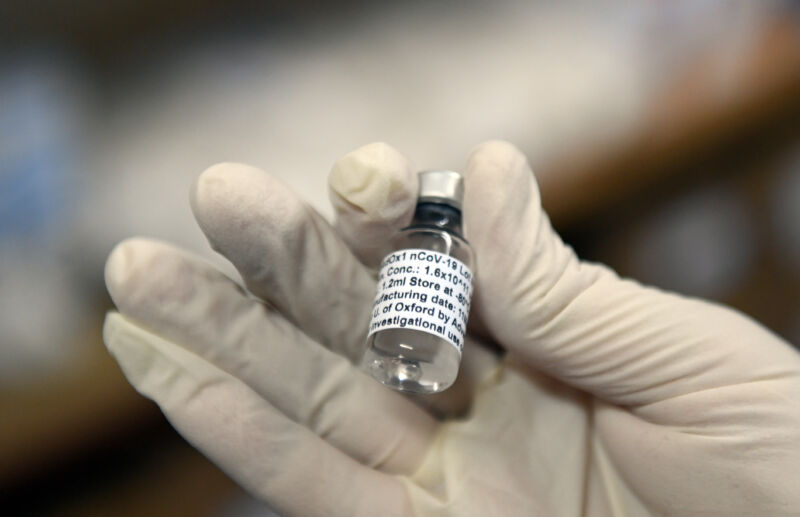
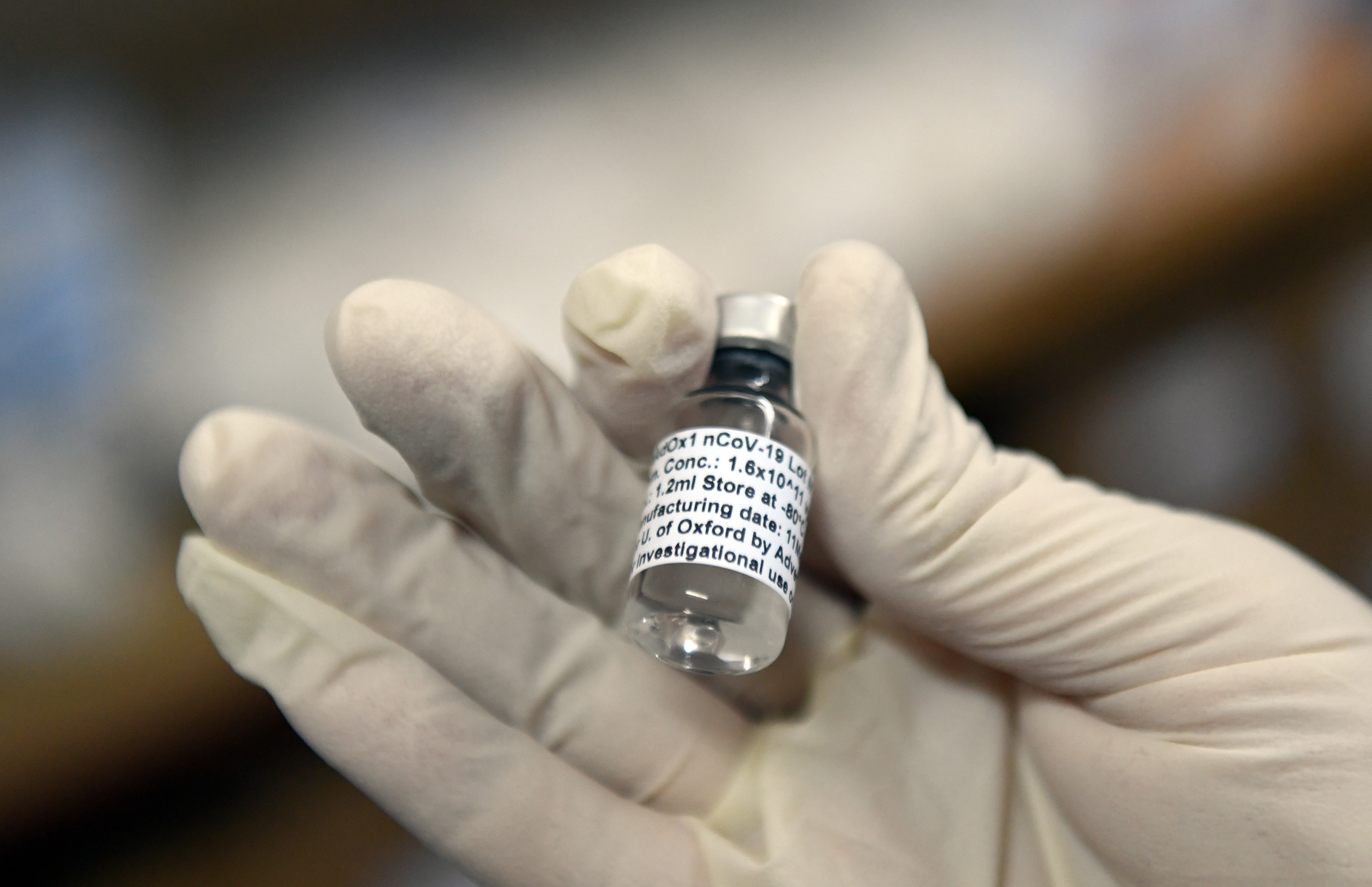
But this is the first mRNA vaccine, and it turns out to be a precious little snowflake. Pfizer’s vaccine has to be stored and shipped at ultracold temperatures, less than 80 degrees below zero—it’ll keep for a few days at higher but still very cold conditions. And it needs vials made of a special glass that’s able to tolerate the freezing temperatures. (This is neat, actually—the key is that the glass is low in boron, exactly the opposite of famously temperature-change-tolerant Pyrex glass, which is a mix of boron and silicon dioxide. The glassmaker Corning has a $204 million contract with the government to make it and cut a deal in May to provide it to Pfizer. Whether Corning can make enough is the tricky part.)
All that shipping and freezing requires a level of technical sophistication that, for now at least, mostly exists in hospitals and labs—posing significant logistical challenges in rural areas and in the developing world. These are the “cold chain” problems that Koff mentioned, the problem of refrigerated shipping. (A critical Ebola vaccine needs the same deep freeze, and engineers stepped up to create specialized coolers to transport it across western Africa—but that was a pandemic that affected tens of thousands of people, not billions, and the people who made the coolers have since gotten out of the cold-chain innovation game.)
“Minus 70 is almost a nonstarter”
Those logistical challenges and an overall shortage of the vaccine are going to limit even further who gets the vaccine first. A spokesperson for Pfizer says the company has built its own network of distribution centers, freezers, and specialized shipping containers. And, meanwhile, Phase I of any vaccination plan will probably involve giving it to health care workers and first responders—the kind of people who’ll have easier access to the places that actually have the drug, and are perhaps more likely to come back for the second shot the Pfizer vaccine requires.
“We understand that Pfizer has a network of locations that it worked with to conduct its clinical trials throughout the United States,” says Anna Legried Dopp, senior director for clinical guidelines and quality improvement at the American Society of Health-System Pharmacists. Dopp says she understands there to be upwards of 100 of these locations. “They’ll leverage the ultracold freezers that were given to them for purposes of the clinical trial,” she says.
This is good; the freezers will be able to change temperatures to accommodate other, future, vaccine candidates that need cold, but not as cold, conditions (like, apparently, Moderna’s).
OK. So at least one set of weaknesses might also be a strength. So might some others. “We’ll probably figure out how to solve, in the short term, the cold chain, just because the estimates of the economic costs I’ve seen in the US are in the trillions of dollars. Longer term, in the US and globally, something that has to be at minus 70 is almost a nonstarter,” says Sam Scarpino, a mathematical epidemiologist at Northeastern University who studies disease spread. “We’ll continue to find out more and more about the vaccine as it scales up from Phase III to being injected in 100 million people, and then a billion people—whether it turns out that there are other things we need out of a vaccine, and if other stuff remains in the pipeline.”
Science by press release
What Scarpino means is, the Pfizer vaccine might be good enough to start healing the world but not good enough to finish the job. Pfizer has promised a peer-reviewed, detailed accounting of results, but for now it’s just a press release, and it leaves a lot out. (Getting science by press release is never ideal.) Pfizer and the FDA withstood extraordinary political pressure to forgo faster-moving data releases that wouldn’t encompass potential side effects, yet the press release didn’t say anything about whether the vaccine shows different levels of protection in different demographic groups (most saliently children, adults, and the elderly) or has longer-term safety issues.
How could it? The vaccine is too new, and studying vaccine efficacy in subgroups is notoriously difficult. But policymakers are going to need that data, because they’re going to have to decide how to deploy limited supplies. If they know one vaccine is better for older people, that helps tell them where to send it—and vaccines will certainly have different skill sets.
For one thing, they’ll have different levels of protection overall. The Pfizer study covered 43,538 people, 38,955 of whom got the two doses required. And the company reported only 94 cases of COVID-19. (Presumably many more of the infected were in the placebo group that didn’t get the actual vaccine; the release didn’t give the exact numbers.) But it’s probably not the case that nine times as many non-vaccinated people got the disease as vaccinated people; those numbers vary based on how many people were in each group. And that math is supposed to include a statistical range of possibility called a confidence interval. It’s sort of the possible answers the same data could account for. The smaller the confidence interval, the more sure that researchers are about a number.
People are going to want those, because they’ll make it easier to compare vaccines. Moderna spokespeople have issued a statement saying they’re about to release their initial data too. What if they say their efficacy is higher than 90 percent? Without a confidence interval, it’ll seem like Moderna’s drug is better than Pfizer’s. But if the confidence intervals of the drugs overlap, people will know that they’re actually closer to each other in terms of effectiveness.
“If Moderna comes out and it’s a 93 percent, let’s say, now we have to unwind the messaging on this. Are these numbers the same? Are they different?” says Peter Bach, director of the Center for Health Policy and Outcomes and the Drug Pricing Lab at Memorial Sloan Kettering Cancer Center. “Sure, it’s a big effect. It’s unmistakable. But because the actual numbers are pretty small, they’re just very unstable.” Confidence intervals will make the public health messaging easier later, when other vaccines come out—especially since nobody’s actually comparing these vaccines head-to-head.
Trial and errors
Comparisons will only happen after the fact, almost inferentially. “It’s very hard to do head-to-head comparisons, in part because nobody’s interested. The companies, unless they see a commercial advantage, aren’t going to do it,” says Arnold Monto, an epidemiologist at the University of Michigan School of Public Health who chairs the FDA’s Vaccines and Related Biological Products Committee. “This information is going to come from observational studies after vaccines are being used.”
At an October meeting of the FDA vaccines committee that Monto chairs, he worried that a too-early reveal of data from any of the companies might induce participants in the study to bail out. When volunteers consent to be part of a trial, they often get the right to leave the study and find out whether they received the vaccine or the placebo. As soon as one seems to work, everyone in every study might, potentially, want to just go get that—torpedoing all the other work in progress. Monto now says he’s a little less worried about that. “It may all be moot, because the trials are large in size,” Monto says. “If people do drop out, it may not really matter in terms of the long-term study of both efficacy and safety.”
In fact, having a working vaccine could, in some interpretations, mean that ethically other companies can’t keep testing their own candidates—exposing people to COVID-19 when, nominally, an actual vaccine exists. That doesn’t seem to be happening either. The other trials are still ongoing. Vaccine makers know how to compare different vaccines against the same disease in “noninferiority” studies. They already do that for influenza shots. COVID-19 vaccines might have entirely different “correlates of protection,” the thing that’s actually conferring immunity. Some might induce more neutralizing antibodies, the immune system’s general infantry, while others might induce more T cells, a more specifically targeted fighter.
“Almost a miracle”
People need vaccines to do different things—to work better on old people or on kids, or to stave off different sets of symptoms. Pfizer’s end points, the things they were actually studying, were bad side effects (which they didn’t see) and a lack of mild symptoms or disease. That seems good, but it’s not the whole story.
“How does that correlate with emergence of symptoms severe enough that they require medical attention? Hospitalization? Mortality? Long-haul symptoms?” asks Llew Keltner, a drug development expert and CEO of Epistat, a health care strategy consultancy. “If we’re preventing hospitalization, preventing death, and preventing long-haul disease at 9 to 1? Oh my God, it’s almost a miracle.” Nobody knows if that’s what the Pfizer vaccine does.
For that matter, a vaccine that has lower efficacy but only requires one dose might be better. Getting two shots is no fun, and it requires an informational infrastructure to track who has gotten what and when. A single shot makes everything easier, even if it works slightly less well. “Maybe we give up a little bit in efficacy,” Bach says, “but true efficacy in the real world with Pfizer and Moderna is hampered, because it’s very hard to get people to return.”
So that’s yet another reason the Pfizer vaccine will encourage rather than block development of competitors. The market, so to speak, isn’t uniform. Two key pieces of information about any vaccine simply aren’t available yet—how long its protection lasts, and whether it prevents not only illness but actual transmission of the disease from person to person.
“I am not concerned about long-term protection initially, because we’ve got a pandemic to deal with. But I think, down the road, duration of protection is going to be very important, given the fact that the virus is not going to go away,” Monto says. “I’ve been around a number of rollouts of vaccines, and the question is always, is this lifelong protection? And we never know the answer until time passes. It’s going to be very difficult to find out, and it’s going to be different for different vaccines.”
We don’t know “longer-term health consequences”
If a vaccine can’t prevent transmission, that may likewise open a door to other candidates. A vaccine that’s 90 percent effective at preventing sickness, in conjunction with all the familiar public health “non-pharmaceutical interventions”—masks, distancing, testing, and contact tracing—might be enough to bring the US back to a new normal by late summer. But it wouldn’t be enough to allow US citizens to travel anywhere that doesn’t have the vaccine. In those places, a vaccinated person exposed to the disease and able to transmit it is just an asymptomatic superspreader.
“In terms of understanding the epidemiological consequences of the vaccine, we don’t know. The longer-term health consequences, we don’t know,” Scarpino says. “The degree to which this actually blocks transmission is going to dictate the kinds of non-pharmaceutical interventions we’ll have to layer with it.”
Even if Pfizer gets some kind of authorization to start giving people shots, as seems likely, the world will still need other COVID-19 vaccines, too. “That was the goal, to not put all our eggs in one basket. In many ways, that’s a good problem to be talking about—how the market will absorb many vaccine candidates. That’s not new to health care,” Dopp says. “Right now, there’s not enough information that would give any sort of picture to that. Right now, people are just wanting to vaccinate with an effective vaccine.” That ember of hope burns on, even with cold water raining down upon it.
This story originally appeared on wired.com.










{kind=link}