As of mid-December, hospitals on average had just 22 percent of their intensive care unit (ICU) beds available across the country, and many were completely full. As the Covid-19 surge continues to intensify, lack of ICU beds can have dire consequences, including not being able to properly care for the sickestpatients, potentially rationing lifesaving care.
But even these bed capacity numbers don’t tell the whole story.
Adding extra critical-care beds in other departments or buildings takes precious time, resources, and space. But adding trained staff is much more difficult, especially deep into a pandemic.
When trained staff are in short supply, it’s even harder for hospitals to best meet the needs of critical-care patients. These patients include people very sick with Covid-19, but also many who need to be in the ICU for other reasons, such as those who have had a heart attack or stroke, are recovering from major surgery, or are sick with the flu, among others.
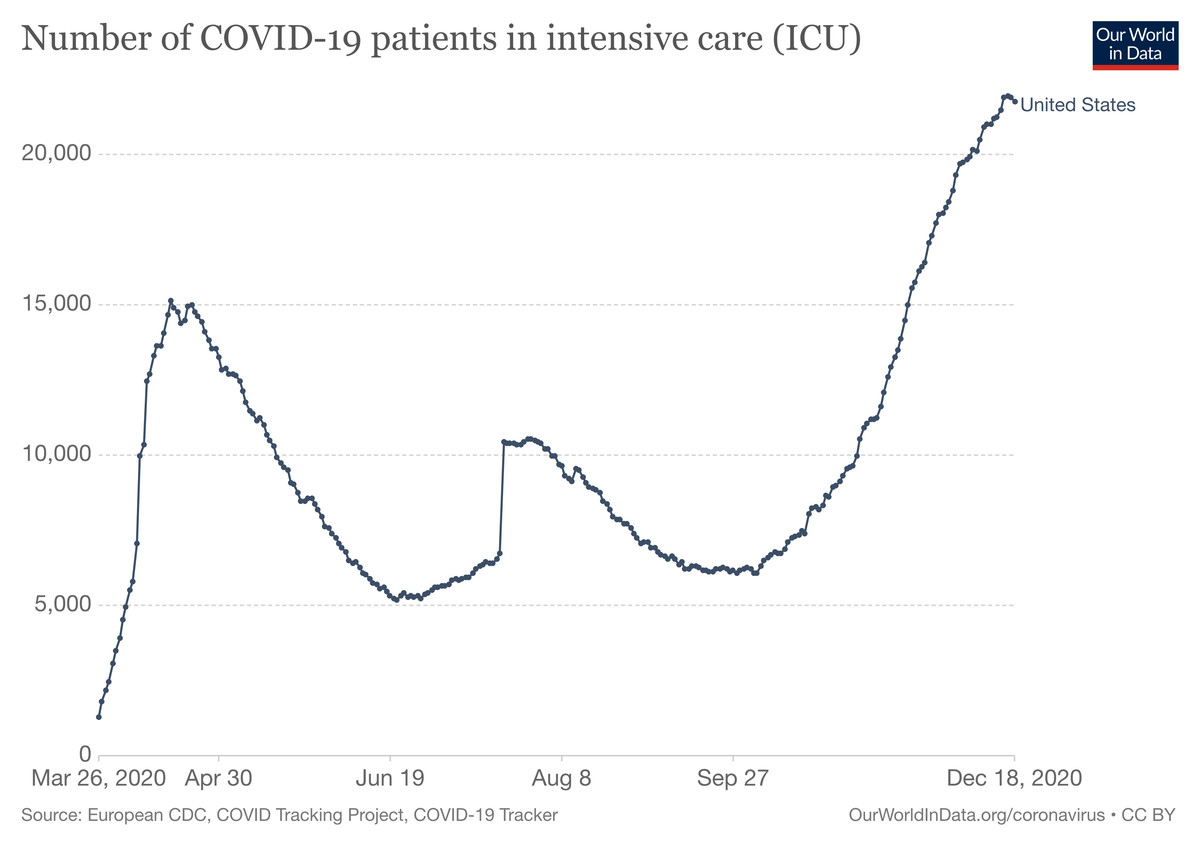
The number of people with Covid-19 currently in the ICU in the US reached an all-time high in mid-November and has been climbing ever since.Our World in Data, with data from COVID Tracking Project and COVID19 Tracker
Only about a dozen states had more than 30 percent ICU capacity left on December 15, and coronavirus case numbers have only accelerated since then. And the reality on the ground in many areas is much worse, as reporting by the New York Times has shown.
From the Times’s data, gathered from the US Department of Health and Human Services, of about 100 hospitals in the Los Angeles area, more than 65 reported ICU occupancy at 90 percent or higher. Cedars-Sinai Medical Center had an occupancy at 112 percent of its capacity.
In Dallas, the fourth-largest metropolitan area in the country, of the 47 hospitals with more than 20 Covid-19 patients, 80 percent of them had zero or just one ICU bed left. The most open beds any hospital had was five.
Nancy Nagle, a pulmonologist and critical-care physician at Integris health system in Oklahoma City, which reported full ICU occupancy in the most recent data to the HHS, says they have turned regular patient rooms into ICU rooms to try to handle the rush of severely ill people. Even so, she said, “occasionally Covid-19 patients must remain in the emergency department for several hours waiting for a bed to become available.”
“Patients keep coming, and we have to take care of them regardless of our staffing levels,” Gisella Thomas, a respiratory therapist at Desert Regional Medical Center in Palm Springs, California, wrote to Vox in an email. “I worry that there is only so long staff can hold up before breaking, which ultimately, in itself, could limit capacity” further.
The sickest Covid-19 patients can linger in the ICU for weeks — or longer. And although we have learned a lot since the spring about how to better treat severely ill Covid-19 patients, the disease itself is still challenging to address, and we don’t have a cure for it. Which means the 2 percent of people who get Covid-19 and end up needing critical care are often in ICUs until either they are able to recover — which often includes invasive intubation treatment — or die.
One of the reasons ICUs have been filling up is that once a patient with Covid-19 gets that sick, they are not likely to stabilize very quickly. A September study found that an average ICU stay for a Covid-19 patient was about a week — almost double the typical stay of 3.8 days for other ICU patients. Other anecdotal reports show that many patients can be in the ICU for weeks or even months. And pinning down this number is crucial for projecting how many beds might be available in the future if cases continue to climb.
As an October study pointed out, if an average length of stay in the ICU is 10 days, that means that every day there is only a 10 percent chance of a new bed opening up. So when admissions exceed that rate, ICUs are likely to get overwhelmed.
This is something those working with critically ill coronavirus patients have to contend with every day. “Covid-19 patients unfortunately stay in the ICU for a long time,” Nagle said. “The course of the disease is very slow, and this contributes to the shortage of available beds.”
And while Covid patients are there, meeting their needs can be extremely labor-intensive. “Covid-19 patients can be incredibly ill, with multiple machines to watch and adjust, multiple medications to give, and lab results to draw and results to watch,” Nagle said. And although we now have a better understanding of possible treatments for seriously ill patients, “patients still respond in varying ways, and their progress and possible outcome is always unpredictable.” This is another reason hospitals don’t always have a good projection for how many ICU beds they might have in the coming weeks or days.
Caring for Covid-19 patients also requires many more steps and precautions than when ICU staff work with other patients, further jamming units. All staff entering an ICU Covid-19 room must don full gowns and PPE each time, which is resource-intensive. “This also creates real difficulties if someone crashes because it slows down our response,” Thomas said. “The need to more thoroughly clean all equipment also creates delays and makes normal staffing levels inadequate for the pandemic.”
In the meantime, doctors, nurses, and other health care workers are struggling to provide the best care they can while being asked to handle more and more patients. “Critically ill patients are very complex,” said Orlando Garner, a pulmonary critical-care physician at Baylor College of Medicine. “There are a lot of moving parts at the same time that require the same amount of priority.” But, he said, “when you are stretched out beyond capacity, you can’t deliver the same quality care unless you create more skilled health care workers, and as we have found out, these are a scarce resource.”
Although hospitals can often somewhat expand the number of beds and amount of supplies, staff are in much shorter supply. “The most precious resource in any hospital are the human beings who are knowledgable and capable of caring for patients,” Sarah Delgado, an acute care nurse practitioner and clinical practice specialist with the American Association of Critical-Care Nurses, wrote to Vox in an email. “It is the limiting factor.” Without enough of these people to care for all of those who are very sick, “patient outcomes are likely to suffer,” she said.
And it is not just ICU physicians and nurses who are in short supply. “Critical care is more of a team sport,” Garner said. “This means physician-delivered care and interventions, but also careful medication selection dosage with pharmacists, skilled nursing care, respiratory therapists, midlevel providers, nutritionists, early mobilization with physical therapists.” To that list, Nagle also adds all of the other hospital staff needed to perform other essential tasks in ICUs, including bathing patients, changing linens, and other functions.
To accommodate surges of very ill Covid-19 patients, many hospitals have had to rework their staffing structure. At Christiana Hospital in Delaware, critical-care nurse Lauren Esposito and her colleagues typically work with critical cardiac patients. But this year, her unit has served as overflow for critical Covid-19 cases. “At first it was a little uneasy,” she wrote for the American Association of Critical-Care Nurses.
Their hospital implemented a tiered staffing strategy in which cardiac nurses would work under trained ICU nurses. “During the shift, if a patient was crashing, we were able to flex and have the ICU nurse go to that patient to provide care,” she wrote. They were also able to provide quick training to nursing staff, for example, on working with intubated patients. Still, the overflow duties were straining, and they weren’t made easier given the intensive isolation these patients are in to stop the spread of infection. “I remember the first time I walked into a patient’s room, it really hits you that you are the primary caregiver and no one else can come in.”
Also, staff now often have to attend to more patients at a time. In California, where last week an average of more than 44,600 people each day tested positive for the coronavirus, Gov. Gavin Newsom dropped the state’s nurse-to-patient ratio from 1:2 to 1:3 in an effort to meet the surging numbers of Covid-19 hospitalizations.
In Oklahoma, Nagle notes that although the ICU nurses she works with usually take care of one to two patients during a shift, “with the shortage of critical-care nurses, each nurse may have three, and under very extreme conditions, even four patients to care for.”
This increase in patients each nurse is seeing — especially in a complex illness like Covid-19 — is a major adjustment. “Nurses are at the patient’s side every hour of every day, administering lifesaving medications, collaborating with other health care team members, translating information to families, and providing end-of-life presence when those families cannot visit due to strict isolation requirements,” Delgado said. “This work cannot be done when the number of patients exceeds staffing capacity.”
And staff themselves often fall ill with the virus. According to a November report, as many as a quarter of Covid-19 infections in some states are among health care workers.
Garner, whose whole family got sick with Covid-19 earlier this year, including his 4-month-old daughter, says getting the illness himself gave him a new perspective on the patients now flooding into local Texas ICUs.
“It could have been me, my wife, or one of my kids on that ICU bed,” he said. “It’s easy to rationalize the amount of sick patients by thinking, ‘oh, well they weren’t distancing,’ or, ‘they weren’t wearing masks,’ but the fact is that nobody deserves to catch this virus and get sick from it, not even the people who doubt it. As the spike continues to grow, compassion is the only thing that can keep us from becoming jaded and burned out.”
The flip side of that is remembering compassion for the health care workers caring for these patients, especially as the holidays approach. Not only will many of these workers continue long shifts through the holidays, they will do so knowing that many people are disregarding public health warnings to avoid gatherings.
“We need the public to do its part,” Delgado said. “Stop nonessential travel, adhere strictly to mask-wearing and social distancing guidelines, and limit gatherings with those outside your household,” Delgado said.
Katherine Harmon Courage is a freelance science journalist and author of Culturedand and Octopus!Find her on Twitter at @KHCourage.
Skinstitut Holiday Gift Kits take the stress out of gifting
Toronto, October 31, 2024 – Beauty gifts are at the top of holiday wish lists this year, and Laser Clinics Canada, a leader in advanced beauty treatments and skincare, is taking the pressure out of seasonal shopping. Today, Laser Clincs Canada announces the arrival of its 2024 Holiday Gift Kits, courtesy of Skinstitut, the exclusive skincare line of Laser Clinics Group.
In time for the busy shopping season, the limited-edition Holiday Gifts Kits are available in Laser Clinics locations in the GTA and Ottawa. Clinics are conveniently located in popular shopping centers, including Hillcrest Mall, Square One, CF Sherway Gardens, Scarborough Town Centre, Rideau Centre, Union Station and CF Markville. These limited-edition Kits are available on a first come, first served basis.
“These kits combine our best-selling products, bundled to address the most relevant skin concerns we’re seeing among our clients,” says Christina Ho, Senior Brand & LAM Manager at Laser Clinics Canada. “With several price points available, the kits offer excellent value and suit a variety of gift-giving needs, from those new to cosmeceuticals to those looking to level up their skincare routine. What’s more, these kits are priced with a savings of up to 33 per cent so gift givers can save during the holiday season.
There are two kits to select from, each designed to address key skin concerns and each with a unique theme — Brightening Basics and Hydration Heroes.
Brightening Basics is a mix of everyday essentials for glowing skin for all skin types. The bundle comes in a sleek pink, reusable case and includes three full-sized products: 200ml gentle cleanser, 50ml Moisture Defence (normal skin) and 30ml1% Hyaluronic Complex Serum. The Brightening Basics kit is available at $129, a saving of 33 per cent.
Hydration Heroes is a mix of hydration essentials and active heroes that cater to a wide variety of clients. A perfect stocking stuffer, this bundle includes four deluxe products: Moisture 15 15 ml Defence for normal skin, 10 ml 1% Hyaluronic Complex Serum, 10 ml Retinol Serum and 50 ml Expert Squalane Cleansing Oil. The kit retails at $59.
In addition to the 2024 Holiday Gifts Kits, gift givers can easily add a Laser Clinic Canada gift card to the mix. Offering flexibility, recipients can choose from a wide range of treatments offered by Laser Clinics Canada, or they can expand their collection of exclusive Skinstitut products.
Brightening Basics 2024 Holiday Gift Kit by Skinstitut, available exclusively at Laser Clincs Canada clinics and online at skinstitut.ca.
Hydration Heroes 2024 Holiday Gift Kit by Skinstitut – available exclusively at Laser Clincs Canada clinics and online at skinstitut.ca.
LONDON (AP) — Most people have accumulated a pile of data — selfies, emails, videos and more — on their social media and digital accounts over their lifetimes. What happens to it when we die?
It’s wise to draft a will spelling out who inherits your physical assets after you’re gone, but don’t forget to take care of your digital estate too. Friends and family might treasure files and posts you’ve left behind, but they could get lost in digital purgatory after you pass away unless you take some simple steps.
Here’s how you can prepare your digital life for your survivors:
Apple
The iPhone maker lets you nominate a “ legacy contact ” who can access your Apple account’s data after you die. The company says it’s a secure way to give trusted people access to photos, files and messages. To set it up you’ll need an Apple device with a fairly recent operating system — iPhones and iPads need iOS or iPadOS 15.2 and MacBooks needs macOS Monterey 12.1.
For iPhones, go to settings, tap Sign-in & Security and then Legacy Contact. You can name one or more people, and they don’t need an Apple ID or device.
You’ll have to share an access key with your contact. It can be a digital version sent electronically, or you can print a copy or save it as a screenshot or PDF.
Take note that there are some types of files you won’t be able to pass on — including digital rights-protected music, movies and passwords stored in Apple’s password manager. Legacy contacts can only access a deceased user’s account for three years before Apple deletes the account.
Google
Google takes a different approach with its Inactive Account Manager, which allows you to share your data with someone if it notices that you’ve stopped using your account.
When setting it up, you need to decide how long Google should wait — from three to 18 months — before considering your account inactive. Once that time is up, Google can notify up to 10 people.
You can write a message informing them you’ve stopped using the account, and, optionally, include a link to download your data. You can choose what types of data they can access — including emails, photos, calendar entries and YouTube videos.
There’s also an option to automatically delete your account after three months of inactivity, so your contacts will have to download any data before that deadline.
Facebook and Instagram
Some social media platforms can preserve accounts for people who have died so that friends and family can honor their memories.
When users of Facebook or Instagram die, parent company Meta says it can memorialize the account if it gets a “valid request” from a friend or family member. Requests can be submitted through an online form.
The social media company strongly recommends Facebook users add a legacy contact to look after their memorial accounts. Legacy contacts can do things like respond to new friend requests and update pinned posts, but they can’t read private messages or remove or alter previous posts. You can only choose one person, who also has to have a Facebook account.
You can also ask Facebook or Instagram to delete a deceased user’s account if you’re a close family member or an executor. You’ll need to send in documents like a death certificate.
TikTok
The video-sharing platform says that if a user has died, people can submit a request to memorialize the account through the settings menu. Go to the Report a Problem section, then Account and profile, then Manage account, where you can report a deceased user.
Once an account has been memorialized, it will be labeled “Remembering.” No one will be able to log into the account, which prevents anyone from editing the profile or using the account to post new content or send messages.
X
It’s not possible to nominate a legacy contact on Elon Musk’s social media site. But family members or an authorized person can submit a request to deactivate a deceased user’s account.
Passwords
Besides the major online services, you’ll probably have dozens if not hundreds of other digital accounts that your survivors might need to access. You could just write all your login credentials down in a notebook and put it somewhere safe. But making a physical copy presents its own vulnerabilities. What if you lose track of it? What if someone finds it?
Instead, consider a password manager that has an emergency access feature. Password managers are digital vaults that you can use to store all your credentials. Some, like Keeper,Bitwarden and NordPass, allow users to nominate one or more trusted contacts who can access their keys in case of an emergency such as a death.
But there are a few catches: Those contacts also need to use the same password manager and you might have to pay for the service.
___
Is there a tech challenge you need help figuring out? Write to us at onetechtip@ap.org with your questions.
The Canadian Paediatric Society says doctors should regularly screen children for reading difficulties and dyslexia, calling low literacy a “serious public health concern” that can increase the risk of other problems including anxiety, low self-esteem and behavioural issues, with lifelong consequences.
New guidance issued Wednesday says family doctors, nurses, pediatricians and other medical professionals who care for school-aged kids are in a unique position to help struggling readers access educational and specialty supports, noting that identifying problems early couldhelp kids sooner — when it’s more effective — as well as reveal other possible learning or developmental issues.
The 10 recommendations include regular screening for kids aged four to seven, especially if they belong to groups at higher risk of low literacy, including newcomers to Canada, racialized Canadians and Indigenous Peoples. The society says this can be done in a two-to-three-minute office-based assessment.
Other tips encourage doctors to look for conditions often seen among poor readers such as attention-deficit hyperactivity disorder; to advocate for early literacy training for pediatric and family medicine residents; to liaise with schools on behalf of families seeking help; and to push provincial and territorial education ministries to integrate evidence-based phonics instruction into curriculums, starting in kindergarten.
Dr. Scott McLeod, one of the authors and chair of the society’s mental health and developmental disabilities committee, said a key goal is to catch kids who may be falling through the cracks and to better connect families to resources, including quicker targeted help from schools.
“Collaboration in this area is so key because we need to move away from the silos of: everything educational must exist within the educational portfolio,” McLeod said in an interview from Calgary, where he is a developmental pediatrician at Alberta Children’s Hospital.
“Reading, yes, it’s education, but it’s also health because we know that literacy impacts health. So I think that a statement like this opens the window to say: Yes, parents can come to their health-care provider to get advice, get recommendations, hopefully start a collaboration with school teachers.”
McLeod noted that pediatricians already look for signs of low literacy in young children by way of a commonly used tool known as the Rourke Baby Record, which offers a checklist of key topics, such as nutrition and developmental benchmarks, to cover in a well-child appointment.
But he said questions about reading could be “a standing item” in checkups and he hoped the society’s statement to medical professionals who care for children “enhances their confidence in being a strong advocate for the child” while spurring partnerships with others involved in a child’s life such as teachers and psychologists.
The guidance said pediatricians also play a key role in detecting and monitoring conditions that often coexist with difficulty reading such as attention-deficit hyperactivity disorder, but McLeod noted that getting such specific diagnoses typically involves a referral to a specialist, during which time a child continues to struggle.
He also acknowledged that some schools can be slow to act without a specific diagnosis from a specialist, and even then a child may end up on a wait list for school interventions.
“Evidence-based reading instruction shouldn’t have to wait for some of that access to specialized assessments to occur,” he said.
“My hope is that (by) having an existing statement or document written by the Canadian Paediatric Society … we’re able to skip a few steps or have some of the early interventions present,” he said.
McLeod added that obtaining specific assessments from medical specialists is “definitely beneficial and advantageous” to know where a child is at, “but having that sort of clear, thorough assessment shouldn’t be a barrier to intervention starting.”
McLeod said the society was partly spurred to act by 2022’s “Right to Read Inquiry Report” from the Ontario Human Rights Commission, which made 157 recommendations to address inequities related to reading instruction in that province.
He called the new guidelines “a big reminder” to pediatric providers, family doctors, school teachers and psychologists of the importance of literacy.
“Early identification of reading difficulty can truly change the trajectory of a child’s life.”
This report by The Canadian Press was first published Oct. 23, 2024.