








")
Here’s an update on COVID-19 cases in Ontario as well as in the greater Kawarthas region.
Ontario is reporting 944 new cases today, the highest daily increase since May 30 when 1,033 cases were reported. The seven-day average of daily cases has increased 16 to 746.
Of Ontario’s 34 health units, 4 are reporting triple-digit increases — Toronto (181), Peel (118), Windsor-Essex (113), and York (112) — with 11 reporting double-digit increases — Hamilton (92), Ottawa (39), Niagara (35), Waterloo (30), Simcoe Muskoka (29), Durham (28), Halton (28), Brant (22), Middlesex-London (21), Wellington-Dufferin-Guelph (19), Chatham-Kent (18) — and 5 reporting no new cases at all.
Of the new cases, 69% are people who have not been fully vaccinated (59% have not received any doses and 10% have received only one dose) and 22% are people who have been fully vaccinated with two doses, with the vaccination status unknown for 9% of the cases because of a missing or invalid health card number.
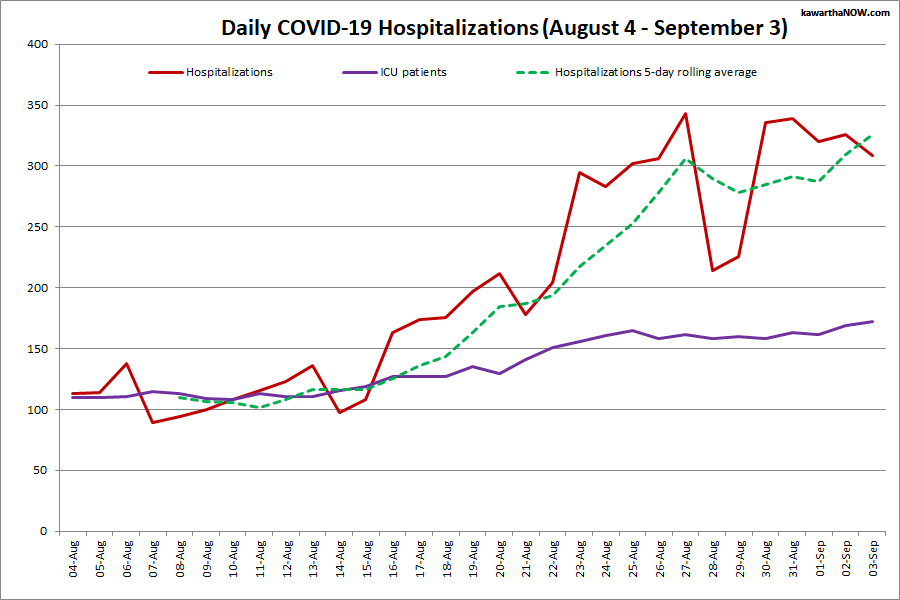
Hospitalizations have decreased by 17 to 309, the number of ICU patients has increased by 3 to 172, and the number of ICU patients on ventilators has decreased by 8 to 97. Ontario is reporting 9 COVID-related deaths, but 5 of these occurred more than 2 months ago and are being reported today as part of a data clean-up, so there were 4 new COVID-related deaths yesterday.
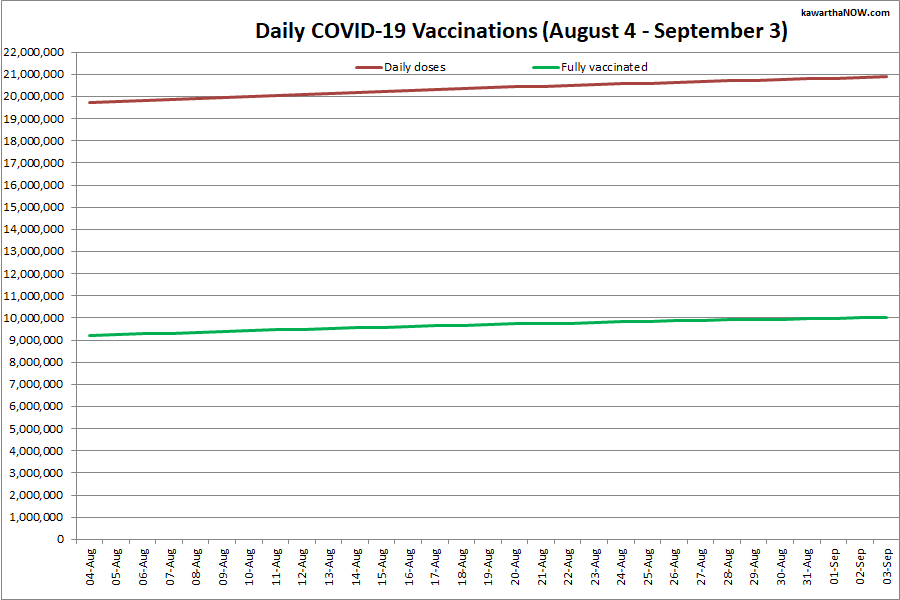
Over 20.9 million vaccine doses have been administered, an increase of 45,886 from yesterday, with over 10 million people fully vaccinated, an increase of 24,636 from yesterday, representing 67.8% of Ontario’s total population.
For a daily summary of cases in Ontario, including a breakdown of cases in each of Ontario’s 34 health units, visit ontario.ca/page/how-ontario-is-responding-covid-19.
Advertisement – story continues below

Advertisement – story continues below
Numbers are unavailable for Peterborough, Kawartha Lakes, Haliburton, Northumberland, and Hastings Prince Edward as the respective health units do not issue reports on weekends. Regional numbers for Saturday, Sunday, and Monday (a statutory holiday) will be included in Tuesday’s update.
As of September 3, there were 66 active cases in the greater Kawarthas region, including 38 in Hastings Prince Edward (17 in Belleville, 12 in Central Hastings, 5 in Quinte West, 3 in Prince Edward County, and 1 in Tyendinaga & Deseronto), 17 in Peterborough, 6 in Kawartha Lakes, and 5 in Northumberland. There are no active cases in Haliburton.
Since the pandemic began in the greater Kawarthas region, there have been 1,694 confirmed positive cases in the Peterborough area (1,655 resolved with 22 deaths), 1,233 in the City of Kawartha Lakes (1,183 resolved with 58 deaths), 972 in Northumberland County (950 resolved with 17 deaths), 127 in Haliburton County (126 resolved with 1 death), and 1,288 in Hastings and Prince Edward counties (1,238 resolved with 12 deaths). The most recent death was reported in Hastings Prince Edward on July 28.
Advertisement – story continues below
For detailed data for each health unit, visit the COVID-19 trackers for Peterborough Public Health, Haliburton, Kawartha, Pine Ridge District Health Unit, and Hastings Prince Edward Public Health.
For more information about COVID-19 in Ontario, visit covid-19.ontario.ca.









